Serum markers of collagen metabolism and serum osteocalcin in relation to pubertal development in 57 boys at 14 years of age
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:

ABSTRACT We investigated whether levels of serum collagen markers and serum osteocalcin are related to pubertal growth and development in a cross-sectional study of 57 healthy boys at 14 y
of age. The level of the soft tissue marker, serum amino-terminal propeptide of type III procollagen(PIIINP) was higher in boys at Tanner stages G3 _versus_ G2(_p_ < 0.01). The levels of
the markers of bone collagen matrix differed only at a more advanced pubertal stage: the formation markers, carboxy-terminal and amino-terminal propeptides of type I procollagen, and the
degradation marker, carboxy-terminal telopeptide of type I collagen were higher only at stage G4 _versus_ G3 (_p_ < 0.01). The marker of bone mineralization, serum osteocalcin was also
higher only at stage G4 _versus_ G3 (_p_ < 0.01). Stage G4 was associated with the pubertal growth spurt. The results demonstrate that pubertal development should be taken into account
when serum levels of collagen markers and osteocalcin are evaluated, and suggest that an increase in serum PIIINP in boys at G3 might predict a normal pubertal growth spurt, but the finding
remains to be confirmed in longitudinal studies. SIMILAR CONTENT BEING VIEWED BY OTHERS ASSOCIATION BETWEEN PUBERTAL TIMING AND BONE AND BODY COMPOSITION IN YOUNG ADULT MEN Article Open
access 19 March 2025 ASSOCIATION BETWEEN SERUM VITAMIN A AND BONE MINERAL DENSITY IN ADOLESCENTS Article Open access 26 February 2025 ASSOCIATIONS BETWEEN PHYSICAL PHYSIQUE/FITNESS IN
CHILDREN AND BONE DEVELOPMENT DURING PUBERTY: A 4-YEAR LONGITUDINAL STUDY Article Open access 04 August 2022 MAIN Body growth and development are accompanied by corresponding changes in
connective tissue growth. Serum markers of the latter (collagen markers) have recently been developed(1), _e.g._ PICP and PINP to reflect synthesis of type I collagen (predominantly in bone)
and ICTP to indicate its degradation. Serum OC levels reflect the rate of mineralization of mature type I collagen(2). PIIINP reflects the synthesis of type III collagen (soft tissues). In
normal boys, height velocity is closely related to the velocity of connective tissue growth, and the effects of estrogens and androgens on bone would be anticipated to strengthen the
correlation between height velocity and the collagen markers. The data on the relationship between bone collagen metabolism and growth during puberty are still scanty and controversial(3–5).
In most previous studies, serum PIIINP(5–7) and serum PICP(3, 4) have been evaluated for age and height velocity, but without reference to pubertal stage. Serum PIIINP, the soft tissue
marker, has been observed to increase at pubertal ages in several studies(5, 6, 8). There are no published data no PINP or ICTP, whereas serum PICP has been observed to increase(3) and, on
the other hand, not to change systematically at pubertal ages(4, 8). We undertook the present study to investigate the relationships of height velocity and pubertal development to serum
collagen markers and serum osteocalcin in 57 healthy boys at 14 y of age. Individual pubertal development was estimated from clinical staging, testicular volume, and serum testosterone
concentration. METHODS This was a cross-sectional study of 57 healthy boys at the same secondary school level in three schools near the Children's Hospital, Helsinki(9). The study was
approved by the parents, the school authorities, and those responsible for school health care, and by the Ethics Committee of the Children's Hospital. Information about the study was
sent to the families. Of the 84 boys, 62 agreed to participate. All the parents and children gave their informed consent. Medical history and physical examination indicated that 60 boys were
healthy; two with bronchial asthma were excluded. There were three dropouts, leaving 57 boys for the study. This cross-sectional study included a physical examination and measurement of
height and weight. Height was measured on a Harpenden scale. Height, similarly measured 6 mo previously(9), was used to calculate height velocity (cm/y). Pubertal development was assessed
from testicular volume. The length and width of the testicles were measured with a ruler to the nearest millimeter. Testicular volume was calculated from the formula: 0.52 × longitudinal
axis in cm × (transverse axis in cm)2(10). The mean testicular volume was used. A cut-off point of 2 mL was used to draw a line between prepuberty and early puberty. Genital stage (G) was
determined according to Tanner(11). The median (range) age of the boys was 13.8(13.0-15.1) y, being similar in boys with different Gs: 13.9 y at G2(_n_ = 9), 13.8 y at G3 (_n_ = 23), 13.7 y
at G4 (_n_= 20), and 13.8 y at G5 (_n_ = 5). A morning blood sample was drawn, and serum was stored at -20 °C until analyzed. Serum testosterone concentration was determined by a RIA(12),
and serum sex hormone-binding globulin concentration with a fluoroimmunoassay (Delfia, Wallac, Turku, Finland). The free androgen index was calculated as total testosterone/sex
hormone-binding globulin × 100. Serum OC levels were determined by a RIA technique (Nichols Institute, San Juan, Capistrano, CA). The sensitivity of the assay is 0.3 μg/L, the intra- and
interassay coefficients being 4.5-6.2% and 4.1-8.9%. Serum PICP, PINP(1, 13). PIIINP(14), and ICTP(15) were measured with RIAs (Orion Diagnostica, Oulunsalo, Finland). The sensitivity of the
PICP assay is 1.2 μ/L, the intra- and interassay coefficients being 2.1-3.7% and 3.5-6.6%. The sensitivity of the PINP assay is 2.3 μg/L, the intra- and interassay coefficients being
2.3-3.5% and 2.5-5.2%. The sensitivity of the ICTP assay is 0.4 μg/L, the intra- and interassay coefficients of variation being 3.8-7.2% and 4.1-7.3%, respectively. Correlations were
calculated using Spearman's rank correlation test. Between-group comparisons were made by Kruskall-Wallis analysis for nonparametric data. After logarithmic transformation of the data
(to obtain Gaussian distribution), multiple _R-_square (explanation rate) was calculated using stepwise regression analysis to evaluate the separate effects of serum testosterone and height
velocity on serum collagen markers. RESULTS _GROWTH AND PUBERTAL STAGE_. Table 1 lists the median values for serum androgen indices and for body growth in the boys at different genital
stages. The differences in testicular volume were significant between the boys at different genital stages, as determined by Tanner staging. Height velocity and serum testosterone level were
higher at more advanced genital stages, the differences being significant between the boys at stages G3 and G4 (_p_ < 0.01). _SERUM LEVELS OF THE MARKERS_. Table 1 lists the median
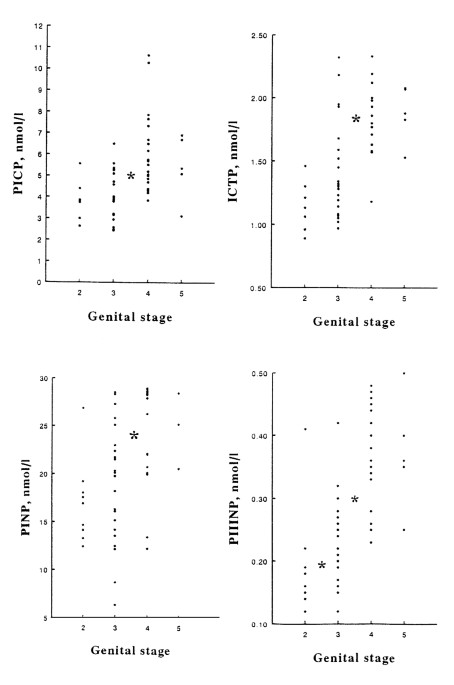
values for the serum markers of collagen metabolism and serum osteocalcin in boys at different genital stages. The serum levels of all the peptides were higher in the boys in advanced
puberty (Fig. 1). The difference in PIIINP was already significant between boys at stages G2 and G3 (_p_ < 0.01), whereas the difference in PICP, PINP, ICTP, and OC levels were
significant only between G3 and G4 (_p_ < 0.01). The PINP levels were about 4-fold as compared with the PICP levels. The serum PINP/PICP molar ratio did not change significantly during
puberty: the medians (range) were 4.7 (3.3-6.4), 4.7 (2.5-7.1), 4.3 (2.7-6.6), and 4.0(3.6-4.3) at G2-G5, respectively. _CORRELATIONS BETWEEN MARKERS_. The serum PICP and PINP levels were
directly related (_r_ = 0.78, _p_ < 0.001). Both PICP and PINP were directly related to PIIINP (_r_ = 0.80 both, _p_< 0.001) and to OC (_r_ = 0.48, _r_ = 0.64, respectively,_p_ <
0.001 both). The PIIINP and OC levels were directly related as well (_r_ = 0.53, _p_ < 0.001). The degradation marker of type I collagen, ICTP, was also directly related to the formation
markers(_p_ < 0.001, all); to PICP and PINP (_r_ = 0.72, both), to PIIINP (_r_ = 0.84), and to OC (_r_ = 0.52). _CORRELATIONS BETWEEN MARKERS, GROWTH, AND PUBERTAL DEVELOPMENT_. Height
velocity, testicular volume, serum testosterone level, and free androgen index were all directly correlated with the serum levels of all the collagen markers and of osteocalcin (Table 2). In
stepwise regression analysis, the variances in PICP, PINP, PIIINP, and OC levels were best explained by the variances in serum testosterone levels, by 44, 47, 60, and 23% (multiple
_R-_square, respectively). Addition of height velocity to the analysis improved the explanation rates of PINP and PIIINP only by 4 and 6%, respectively, and did not improve the explanation
rate of PICP or OC. The variance in ICTP was best explained, by 51%, by the variance in height velocity, and addition of serum testosterone levels to the analysis improved it only by a
further 5%. DISCUSSION Hypogonadism with long-standing testosterone deficiency is known to be associated with osteoporosis(16). However, the data on the relationship of androgens and the
bones are scanty(17). The present study evaluated the relationship between bone and soft tissue collagen metabolism and pubertal development in boys. Bone matrix is formed by type I collagen
fibers and noncollagenous proteins, which are later mineralized(18). During type I collagen synthesis, the amino- and carboxy-terminal propeptides PICP and PINP are cleaved off from the
larger procollagen proteins(19) and during its degradation the cross-links between the collagen molecules, _e.g._ ICTP, are separated(1). The serum levels of PICP and ICTP, respectively,
have been observed to correlate with bone formation and resorption(20). Levels of serum PICP(3, 4, 8) and the soft tissue collagen formation marker, serum PIIINP, have been observed(5–8) to
correlate with height velocity. In the present study, type I collagen synthesis was evaluated with two markers, PICP and the novel marker PINP, and degradation with ICTP, in boys of the same
age but at different pubertal stages. The results of this cross-sectional study demonstrate that the serum markers of collagen metabolism and of mineralization are associated not only with
body growth but also with pubertal development. All the markers correlated positively with height velocity, with the traditional Tanner staging, with serum testosterone concentration, and
with testicular volume. In the present study, the ratio of the serum molar levels of the amino-terminal to the carboxy-terminal propeptides of type I collagen was about 4-fold. This may be
due to differences in the catabolism of these peptides; PICP being cleared mainly via mannose(21) and PINP via scavenger receptors in the liver(22). The receptors may be differently
sensitive to hormones, for in some studies glucocorticoids seem to up-regulate the mannose receptors(23), whereas they do not seem to affect the scavenger receptors(24). The unchanged
PINP/PICP ratio at different pubertal stages argues against an effect of testosterone in their clearance In the present study, higher serum PIIINP levels were observed in boys at stages G3
_versus_ G2. Significant differences in PICP, PINP, ICTP, and OC were observed between boys only at stages G3 and G4. This was accompanied with a significant difference in serum testosterone
levels and height velocity. These results suggest that, in early puberty, adrenal androgens may play a role in the growth of soft tissues, before testosterone production increases, and may
then stimulate the later pubertal bone growth spurt. An increase in serum PIIINP level has been suggested to predict a good response in height velocity in children during growth hormone
treatment(6). Our results suggest that an increase in serum PIIINP in boys at stage G3 may predict a normal pubertal growth spurt, but the finding remains to be confirmed in longitudinal
studies. In multiple stepwise regression analysis, the variance in ICTP was best explained by the variance in height velocity. In contrast, the variance in the other markers was best
explained by the variation in serum testosterone levels. The results suggest independent roles for serum testosterone in the formation of bone and soft tissues, and in addition, emphasize
the close association between increased degradation and remodeling of bone (ICTP) and the growth of the skeleton (height velocity). The present study did not allow for the evaluation of the
effect of growth hormone secretion in pubertal growth. The direct relationship between serum testosterone and the type I collagen peptide levels in the boys of the present study contrasts
with the inverse relationship between serum estradiol and bone turnover markers observed in girls(25). This may be attributed to the differences in the timing of the peak peptide levels: in
boys the peak is found in advanced puberty, when serum testosterone levels are higher, whereas in girls it occurs in early puberty, when serum estradiol levels are still continuing to
rise(25). The causes are unknown, as the regulation of bone metabolism in puberty is still unclear, but the inverse relationship between serum estradiol and the peptides may reflect an
appropriate decrease in tissue sensitivity to sex steroids by the end of body growth. OC is a noncollagenous protein of bone synthesized by osteoblasts and incorporated into the bone
matrix(26, 27). Serum OC levels possibly reflect the bone mineralization rate(2). Serum OC levels have mostly been evaluated in relation to age and height velocity(28–31), but ignoring
pubertal stage. Serum OC levels are higher in children than in adults(32) and the levels correlate with skeletal growth in children(28, 29). An association between pubertal development and
bone mineralization has been demonstrated in other ways: bone mineral density was lower in boys with constitutional delay of puberty(33) and in adult males with such a history(33). The wide
variation in timing of puberty may be critical for the development of peak bone mineral density(17, 33–35). The present study, showing peak OC levels at Tanner stage G4, suggests a parallel
timing of maximal bone matrix formation and mineralization of bone in boys at puberty. The regulation of bone mineralization is still unclear: in the present study only 23% of the variance
in serum OC was explained by the variation in serum testosterone levels, and addition of height velocity in the analysis did not improve the explanation rate at all. The results of this
cross-sectional study suggest that pubertal development in boys should be taken into account when serum levels of collagen markers and osteocalcin are evaluated. The serum level of PIIINP,
the soft tissue collagen marker, was already higher in boys at stage G3 _versus_ G2, whereas the markers of the bone collagen matrix, serum PICP, PINP, and ICTP, and the marker of bone
mineralization, OC, were not higher until stage G4_versus_ G3. The latter differences were associated with the pubertal growth spurt. The results suggest that an increase in serum PIIINP in
boys at stage G3 may predict a normal pubertal growth spurt, but the finding remains to be confirmed in longitudinal studies. ABBREVIATIONS * ICTP: carboxy-terminal telopeptide of type I
collagen * G: Tanner's genital stage * OC: osteocalcin * PICP: carboxy-terminal propeptide of type I procollagen * PIIINP: amino-terminal propeptide of type III procollagen * PINP:
amino-terminal propeptide of type I procollagen REFERENCES * Risteli L, Risteli J 1993 Biochemical markers of bone metabolism. _Ann Med_ 25: 385–293. Article CAS PubMed Google Scholar *
Charles P, Hasling C, Risteli L, Risteli J, Mosekilde L, Eriksen EF 1992 Assessment of bone formation by biochemical markers in metabolic bone disease: separation between osteoblastic
activity at the cell and tissue level. _Calcif Tissue Int_ 51: 406–411. Article CAS PubMed Google Scholar * Saggese G, Bertelloni Baroncelli GI, DiNero G 1992 Serum levels of
carboxyterminal propeptide of type I procollagen in healthy children from the 1st year of life to adulthood and in metabolic bone diseases. _Eur J Pediatr_ 151: 764–768. Article CAS PubMed
Google Scholar * Trivedi P, Risteli J, Risteli L, Hindmarsh PC, Brook CGD, Mowat AP 1991 Serum concentrations of the type I and III procollagen propeptides as biochemical markers of
growth velocity in healthy infants and children and in children with growth disorders. _Pediatr Res_ 30: 276–280. Article CAS PubMed Google Scholar * Danne T, Gruters A, Schuppan D,
Quantas N, Enders I, Weber B 1989 Relationship of procollagen type III propeptide-related antigens in serum to somatic growth in healthy children and patients with growth disorders. _J
Pediatr_ 114: 257–260. Article CAS PubMed Google Scholar * Trivedi P, Hindmarsh P, Risteli J, Risteli L, Mowat A, Brook CGD 1989 Growth velocity, growth hormone therapy, and serum
concentrations of the amino-terminal propeptide of type III procollagen. _J Pediatr_ 114: 225–230. Article CAS PubMed Google Scholar * Lindqvist U, Laurent TC 1992 Serum hyaluronan and
aminoterminal propeptide of type III procollagen: variation with age. _Scand J Clin Lab Invest_ 52: 613–621. Article CAS PubMed Google Scholar * Hertel NT, Stoltenberg M, Juul A, Main
KM, Muller J, Nielsen CT, Lorentzen I, Skakkebaek NE 1993 Serum concentrations of type I and type III procollagen propeptides in healthy children and in girls with central precocious puberty
during treatment with gonadotropin-releasing hormone analog and cyproterone acetate. _J Clin Endocrinol Metab_ 76: 924–927. CAS PubMed Google Scholar * Anttila R, Koistinen R, Seppälä M,
Koistinen H, Siimes MA 1994 Insulin-like growth factor I and insulin-like growth factor binding protein 3 as determinants of blood hemoglobin concentration in healthy subjects. _Pediatr
Res_ 36: 745–748. Article CAS PubMed Google Scholar * Hansen P, With TK 1952 Clinical measurements of testes. _Acta Med Scand Suppl_ 206: 457–465. Google Scholar * Tanner JM, Whitehouse
RH 1965 Clinical longitudinal standards for height, weight, height velocity, weight velocity and stages of puberty. _Arch Dis Child_ 51: 170–179. Article Google Scholar * Apter D, Jänne
O, Karvonen P, Vihko R 1976 Simultaneous determination of five sex hormones in human serum by radioimmunoassay after chromatography on Lipidex-5000. _Clin Chem_ 22: 32–38. CAS PubMed
Google Scholar * Melkko J, Niemi S, Risteli L, Risteli J 1990 Radioimmunoassay of the carboxyterminal propeptide of human type I procollagen. _Clin Chem_ 36: 1328–1332. CAS PubMed Google
Scholar * Risteli J, Niemi S, Trivedi P, Mäentausta O, Mowat AP, Risteli L 1988 Rapid equilibrium radioimmunoassay for the aminoterminal propeptide of human type III procollagen. _Clin
Chem_ 34: 715–718. CAS PubMed Google Scholar * Risteli J, Elomaa I, Niemi S, Novamo A, Risteli L 1993 Radioimmunoassay for the pyridinoline cross-linked carboxy-terminal telopeptide in
metabolic bone disease: correlation with bone of type I collagen: a new serum marker of bone collagen degradation. _Clin Chem_ 39: 635–640. CAS PubMed Google Scholar * Jackson JA,
Kleerekoper M, Parfitt AM, Rao DS, Villenueva AR, Frame B 1987 Bone histomorphometry in hypogonadal and eugonadal men with spinal osteoporosis. _J Clin Endocrinol Metab_ 65: 53–58. Article
CAS PubMed Google Scholar * Vanderschueren D, Bouillon R 1995 Androgens and bone. _Calcif Tissue Int_ 56: 341–346. Article CAS PubMed Google Scholar * Prockop DJ, Kivirikko KI,
Tuderman L, Guzman NA 1979 The biosynthesis of collagen and its disorders. _N Engl J Med_ 301: 77–85. Article CAS PubMed Google Scholar * Prockop DJ, Kivirikko KI, Tuderman L, Guzman NA
1979 The biosynthesis of collagen and its disorders. _N Engl J Med_ 301: 13–23. Article CAS PubMed Google Scholar * Eriksen EF, Charles P, Melsen F, Mosekilde L, Risteli L 1993 Serum
markers of type I collagen formation and degradation in metabolic bone disease: correlation with histomorphometry. _J Bone Miner Dis_ 8: 127–132. Article CAS Google Scholar * Smedsrod B,
Melkko J, Risteli L, Risteli J 1990 Circulating C-terminal propeptide of type I procollagen is cleared mainly via the mannose receptor in liver endothelial cells. _Biochem J_ 271: 345–350.
Article CAS PubMed PubMed Central Google Scholar * Melkko J, Hellevik T, Risteli L, Risteli J, Smedsrod B 1994 Clearance of NH2-terminal propeptides of type I and III procollagen is a
physiological function of the scavenger receptor in liver endothelial cells. _J Exp Med_ 179: 405–412. Article CAS PubMed Google Scholar * Cowan HB, Vick S, Conary JT, Shepherd VL 1992
Dexamethasone up-regulates mannose receptor activity by increasing mRNA levels. _Arch Biochem Biophys_ 296: 314–320. Article CAS PubMed Google Scholar * Hansen M, Stoltenberg M, Host NB,
Lorenzen I, Bentsen KD 1995 Glucocorticoids inhibit the synthesis of type III collagen, but do not affect the hepatic clearance of its aminoterminal propeptide (PIIINP). _Scand J Clin Lab
Invest_ 55: 543–548. Article CAS PubMed Google Scholar * Blumsohn A, Hannon RA, Wrate R, Barton J, Al-Dehaimi AW, Colwell A, Eastell R 1994 Biochemical markers of bone turnover in girls
during puberty. _Clin Endocrinol_ 40: 663–670. Article CAS Google Scholar * Price PA, Parthermore JG, Deftos LJ 1980 New biochemical marker for bone metabolism. Measurement by
radioimmunoassay of bone GLA protein in the plasma of normal subjects and patients with bone disease. _J Clin Invest_ 66: 878–883. Article CAS PubMed PubMed Central Google Scholar *
Delmas PD 1992 Clinical use of biochemical markers of bone remodeling in osteoporosis. _Bone Suppl_ 13: 17–22. Article Google Scholar * Tarallo P, Henny J, Fournier B, Siest G 1990 Plasma
osteocalcin: biological variations and reference limits. _Scand J Lab Invest_ 50: 649–655. Article CAS Google Scholar * Sidenius Johansen J, Giwercman A, Hartwell D, Nielsen CT, Price PA,
Christiansen C 1988 Serum bone GLA-protein as a marker of bone growth in children and adolescents: correlation with age, height, serum insulin-like growth factor I, and serum testosterone.
_J Clin Endocrinol Metab_ 67: 273–278. Article Google Scholar * Lian JB, Gundberg CM 1988 Osteocalcin. Biochemical considerations and clinical applications. _Clin Orthop Res_ 226: 267–280.
CAS Google Scholar * Magnusson P, Häger A, Larsson L 1995 Serum osteocalcin and bone and liver alkaline phosphatase isoforms in healthy children and adolescents. _Pediatr Res_ 38:
955–961. Article CAS PubMed Google Scholar * Gundberg CM, Lian JB, Gallop PM 1983 Measurements ofγ-carboxyglutamate and circulating osteocalcin in normal children and adults. _Clin Chim
Acta_ 128: 1–8. Article CAS PubMed Google Scholar * Bertelloni S, Baroncelli GI, Battini R, Perri G, Saggese G 1995 Short-term effect of testosterone treatment on reduced bone density in
boys with constitutional delay of puberty. _J Bone Miner Res_ 10: 1488–1495. Article CAS PubMed Google Scholar * Finkelstein JS, Neer RM, Biller BMK, Crawford JD, Klibanski A 1992
Osteopenia in men with a history of delayed puberty. _N Engl J Med_ 326: 600–604. Article CAS PubMed Google Scholar * Shaw NJ, Bishop NJ 1995 Mineral accretion in growing bones-a
framework for the future. _Arch Dis Child_ 72: 177–179. Article CAS PubMed PubMed Central Google Scholar Download references AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of
Allergic Diseases, Helsinki, Finland Ritva Sorva & Markku Turpeinen * Department of Allergic Diseases the Children's Hospital, Helsinki, Finland Raija Anttila, Martti A Siimes &
Antti Sorva * University of Helsinki, Antti Sorva * Malmi Hospital, Helsinki, Finland Antti Sorva * Department of Clinical Chemistry, University of Helsinki, and United Laboratories,
Helsinki, Finland Riitta Tähtelä Authors * Ritva Sorva View author publications You can also search for this author inPubMed Google Scholar * Raija Anttila View author publications You can
also search for this author inPubMed Google Scholar * Martti A Siimes View author publications You can also search for this author inPubMed Google Scholar * Antti Sorva View author
publications You can also search for this author inPubMed Google Scholar * Riitta Tähtelä View author publications You can also search for this author inPubMed Google Scholar * Markku
Turpeinen View author publications You can also search for this author inPubMed Google Scholar ADDITIONAL INFORMATION Supported by the Emil Aaltonen Foundation, Tampere, Finland. RIGHTS AND
PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Sorva, R., Anttila, R., Siimes, M. _et al._ Serum Markers of Collagen Metabolism and Serum Osteocalcin in Relation
to Pubertal Development in 57 Boys at 14 Years of Age. _Pediatr Res_ 42, 528–532 (1997). https://doi.org/10.1203/00006450-199710000-00018 Download citation * Received: 11 June 1996 *
Accepted: 11 February 1997 * Issue Date: 01 October 1997 * DOI: https://doi.org/10.1203/00006450-199710000-00018 SHARE THIS ARTICLE Anyone you share the following link with will be able to
read this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing
initiative