Use of near-infrared imaging using indocyanine green associates with the lower incidence of postoperative complications for intestinal and mesenteric injury
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:

ABSTRACT Anastomotic leakage after intestinal resection is one of the most serious complications of surgical intervention for hollow viscus injury. Adequate vascular perfusion of the
anastomotic site is essential to prevent anastomotic leakage. Near-infrared imaging using indocyanine green (NIR-ICG) is useful for the objective assessment of vascular perfusion. The aim of
this study was to evaluate the association of NIR-ICG with intestinal and mesenteric injuries. This was a retrospective, single-center study of patients undergoing surgery for intestinal
and mesenteric injuries. NIR-ICG was used to evaluate vascular perfusion. Postoperative complications were assessed between NIR-ICG and non-NIR-ICG groups.The use of NIR-ICG was associated
with a lower incidence of Clavien-Dindo grade ≥ III complications with a statistical tendency (p = 0.076). When limited to patients that underwent intestinal resection, the use of NIR-ICG
was significantly associated with a lower risk of perioperative complications (p = 0.009). The use of NIR-ICG tended to associate with the lower incidence of postoperative complications
after intestinal and mesenteric trauma surgery. NIR-ICG was associated with a significantly lower risk of complications in patients undergoing intestinal resection. The NIR-ICG procedure is
simple and quick and is expected to be useful for intestinal and mesenteric trauma. SIMILAR CONTENT BEING VIEWED BY OTHERS ASSESSMENT OF GASTRIC POUCH BLOOD SUPPLY WITH INDOCYANINE GREEN
FLUORESCENCE IN CONVERSIONAL AND REVISIONAL BARIATRIC SURGERY: A PROSPECTIVE COMPARATIVE STUDY Article Open access 06 June 2023 ADDED VALUE OF POSITIVE INTRALUMINAL CONTRAST CT OVER
FLUOROSCOPIC EXAMINATION FOR DETECTING GASTROINTESTINAL LEAKAGE AFTER GASTROINTESTINAL SURGERY Article Open access 10 January 2024 INFLUENCE OF INTRAOPERATIVE VASOPRESSOR USE ON INDOCYANINE
GREEN FLUORESCENCE ANGIOGRAPHY: FIRST EVALUATION IN AN EXPERIMENTAL MODEL Article Open access 06 May 2021 INTRODUCTION Early surgical intervention is essential for the management of hollow
viscus injury (HVI). A delay in diagnosis and treatment results in peritonitis, hemodynamic instability, and increased mortality and morbidity rates1,2,3,4. However, because the incidence of
HVI after blunt abdominal trauma is low, surgeons have limited experience in managing these injuries5. Surgical interventions for HVI are associated with several complications. Anastomotic
leakage (AL) after intestinal resection, especially colocolic or colorectal anastomosis, is one of the most serious and potentially life-threatening post-operative complications which has
been reported to occur in 2.5%–6.6% of colonic injuries6,7. Adequate vascular perfusion to the anastomotic site is important to prevent AL8,9. One technique commonly used to assess regional
intestinal vascular perfusion is subjective clinical assessment by the surgeon performing the procedure, including evaluation of the color of the serosa and mucosa, bleeding at the bowel
edge, beating of the mesenteric vessels, and bowel peristalsis. However, the accuracy of this method is limited as it is strongly influenced by the surgeon's personal experience and
other external factors10. Further, subjective assessment of vascular perfusion may be difficult during acute mesenteric ischemia, and the accuracy of intestinal survival prediction using
only clinical criteria was as low as 57.7%11,12. In contrast, near-infrared (NIR) imaging using indocyanine green (ICG) (NIR-ICG) is useful for the objective assessment of vascular
perfusion13. The use of this tool could increase the accuracy of assessment of vascular perfusion status and reduce complications compared to clinical assessment. To our knowledge, however,
there have been no reports on the effectiveness of NIR-ICG to prevent complications associated with intestinal and mesenteric injuries. Thus, the aim of this study was to evaluate the
association of NIR-ICG with postoperative complications after surgery for intestinal and mesenteric injury. RESULTS Among the trauma patients transported to our hospital, 37 patients with
abdominal trauma who required surgery for intestinal or mesenteric injury were included in this study. The NIR-ICG group included 11 patients, and the non-NIR-ICG group included 26 patients.
The baseline characteristics of both groups are presented in Table 1. As the prevalence of male trauma cases was three times higher than that of females, NIR-ICG was only used in male
patients. There was no difference in the mechanism of injury or the type of trauma between the two groups, and the AAST grade was significantly higher in the NIR-ICG group (p < 0.01).
Regarding vital signs on admission, heart rate was higher in the non-NIR-ICG group, but there was no difference in indicators of circulatory failure including systolic blood pressure, base
excess, or lactate levels between the two groups. The sites of trauma were the colon (one patient), small bowel (2 patients), colon and mesenteric hematoma or injury (5 patients), small
bowel and mesenteric hematoma or injury (13 patients), mesenteric hematoma or injury (15 patients), and small bowel, colon and mesenteric injuries (one patient). Regarding AAST grading for
small and large bowel injury, there were 16, 4, and 2 cases of grade 2, grade 3, and grade 5 injuries, respectively. Table 2 summarizes the postoperative complications of the NIR-ICG group
and the non-NIR-ICG group. The overall rate of Clavien-Dindo (CD) grade ≥ III complications was 24.3% (9/37) and all cases were in the non-NIR-ICG group (p = 0.036). The complications
included surgical site infection (SSI) in 4 cases, paralytic ileus in 2 cases, AL in 1 case, adhesive obstruction and short bowel syndrome (SBS) in 1 case, and pancreatic fistula in 1 case.
Pancreatic fistula was caused by pancreatic injury and was excluded when examining the efficacy of NIR-ICG used to assess intestinal vascular perfusion. When limited to intestinal-related
complications, the incidence of CD grade ≥ III was 21.6% (8/37), and all the cases occurred in the non-NIR-ICG group (p = 0.076). When limited to intestinal complications, the rate of CD
grade ≥ II complications was 16.2% (6/37), and all cases occurred in the non-NIR-ICG group (p = 0.151). The complications included paralytic ileus in 4 cases, AL in 1 case, and adhesive
obstruction and SBS in 1 case. Seventeen patients required intestinal resection. All complications of CD grade ≥ III and intestinal complications of CD grade ≥ II only occurred in the
non-NIR-ICG group (CD grade ≥ III: 35.3% (6/17), p = 0.009; CD grade ≥ II: 23.5% (4/17), p = 0.08). In the NIR-ICG group, only one patient had CD grade I paralytic ileus, but no other
complications were observed (Table 3). There were no complications due to the use of ICG, and no patients in this group experienced a delay in oral intake or prolonged hospital stay.
DISCUSSION This study showed that the use of NIR-ICG tended to associate with the lower incidence of CD grade ≥ III complications (p = 0.076). No CD grade ≥ II intestinal complications were
observed in the NIR-ICG group. When limited to the group that underwent intestinal resection, the use of NIR-ICG significantly associated with the lower incidence of postoperative
complications (p = 0.009). Paralytic ileus was common in the non-NIR-ICG group. It is possible that a failure to identify poor vascular perfusion through subjective evaluation in this group
resulted in slowing of intestinal peristalsis and paralytic ileus. In the intestinal resection group, four cases of SSIs with CD grade ≥ II were observed. All patients were in the
non-NIR-ICG group. By evaluating vascular perfusion with NIR-ICG, it may be possible to avoid unnecessary intestinal resection and reduce the risk of SSI due to contamination. AL is one of
the most serious complications after intestinal resection for HVI, with a reported incidence of 2.5%–6.6% of all colonic injuries6,7. In addition, emergency resection is an independent risk
factor for AL (relative risk 4–6, 95% confidence interval 1.9–9.8). The presence of peritonitis is also a predictor of AL14. Since trauma patients who require emergency surgery are presumed
to be at high risk for AL, preventive measures should be implemented. Previous studies have reported that vascular perfusion is important for reducing AL8,9. Compared to the less reliable
subjective assessments12, objective confirmation of good vascular perfusion in the resected bowel stump by NIR-ICG may help prevent complications due to impaired vascular perfusion.
Considering the incidence of AL reported so far, further studies are needed to evaluate the efficacy of NIR-ICG for HVI. AL increases mortality, length of hospital stay, 30-day readmission,
and postoperative infection rates14,15,16,17. As a result, hospital costs increased by more than $25,000 in the United States17 and more than €50,000 in Europe18 when compared to low-cost
ICG. Complications, not limited to AL, doubled the length of hospital stay, increased the average total cost by $25,000, and decreases total balance and turns negative, resulting in a large
loss19. In addition, treatment of SBS requires long-term infusions, leading to an increased risk of infection and increased cost and mortality20. The same is true for SSI, which has
disadvantages such as prolonged hospital stay, increased costs, and prolonged use of antimicrobials21. We believe that the use of NIR-ICG will reduce the risk of these complications and
their associated consequences. A few studies have also investigated the use of NIR-ICG for brain injuries and burns. However, there are no reports of its use in torso trauma and to the best
of our knowledge, this is the first report using NIR-ICG for intestinal and mesenteric injury. The use of NIR-ICG has made it possible to objectively evaluate intestinal vascular perfusion,
which was previously evaluated using subjective evaluation of mucosal color, mesenteric vascular pulsation, and intestinal peristalsis8. An objective evaluation of intestinal vascular
perfusion can ensure sufficient perfusion at the intestinal anastomosis and avoid unnecessary intestinal resection, which may reduce the incidence of complications caused by intestinal and
mesenteric injuries, such as AL and SSI. In addition to improving patient outcomes, this could shorten hospital stays, reduce costs, and optimize the use of antimicrobials. NIR-ICG has
several advantages including the ability to perform rapid evaluation of vascular perfusion within 60 s in real-time using a simple technique, and the ability to record images allowing for
retrospective evaluation. Achieving hemostasis is the mainstay of treatment in hemodynamically unstable patients. NIR-ICG should be performed in patients with stable disease. The results of
this study demonstrate the feasibility of NIR-ICG in patients with intestinal and mesenteric injury with stable hemodynamics after emergency surgery. This study has several limitations worth
noting. First, this was a retrospective, single-center study; as this was not a randomized controlled trial, the selection bias could not be ruled out and we could not confirm the
effectiveness of NIR-ICG. Second, our selection of patients was based on the surgeon’s evaluation. Thus, we could not exclude the possibility of categorizing a patient that did not show any
impaired perfusion parameters and thereby, be considered a negative control in patients with normal bowel perfusion following mesenteric resection. Third, the number of included patients was
small and further studies with a large study population warranted to validate our results. In this study, the NIR-ICG group included only males, and so randomization for gender differences
is also needed. Fourth, factors other than vascular perfusion might be the cause of intestinal complications such as AL. Future studies should consider the association of other traumatic
sites, operator factors, and preoperative nutritional status on the risk of intestinal complications. Fifth, the factors affecting vascular perfusion should be considered. Although none of
the patients in the present study had undergone multiple abdominal surgeries in the past, the effect of multiple previous abdominal surgeries on the fluorescence intensity of ICG cannot be
denied. In addition, it might be necessary to examine whether the size of the resected mesentery affects vascular perfusion evaluation. Sixth, the delayed outflow type was not examined in
this study. Thus, we could not exclude the possibility of a bias, which could be attributed to a different type of perfusion mode. Seventh, a difference in the proportion of complications
among subgroups was significant but underpowered, due to a limited sample size. Finally, due to the diverse background of trauma, the protocol for using NIR-ICG has not been determined.
Therefore, multi-institutional randomized studies are needed to confirm whether NIR-ICG can reduce complications such as the AL rate in intestinal mesenteric injury. METHODS STUDY DESIGN
This was a retrospective, single-center study of patients undergoing surgery due to intestinal and mesenteric injuries from December 2006 to March 2021. This observational study protocol was
reviewed and approved by the Institutional Review Board, the Ethics Committee of the Yokosuka Kyosai Hospital (No. 18-14). The Ethics Committee of the Yokosuka Kyosai Hospital also approved
that; the requirement for written informed consent was waived; and the individual informed consent was opted out, due to a nature of retrospective study design, per the Personal Information
Protection Law and National Research Ethics Guideline in Japan. The study was conducted in accordance with the principles of the Declaration of Helsinki. The following patient data were
collected from clinical records: age, sex, vital signs, blood test results, characteristics and mechanism of injury, severity of intestinal injury, length of hospital stay, days until oral
intake and postoperative complications. The inclusion criteria were (1) cases of blunt or penetrating injuries and (2) cases diagnosed with intestinal injury or mesenteric injury before or
during surgery. NEAR-INFRARED IMAGING USING INDOCYANINE GREEN13 ICG is a water-soluble compound with a molecular weight of 774.96 Da and fluorescent properties. ICG binds to serum proteins
that are taken up by liver cells and excreted in bile; therefore, it is widely used clinically as a test drug for hepatic and circulatory functions. ICG contains iodine and is
contraindicated in patients with iodine hypersensitivity; however, it is a relatively safe reagent with low toxicity and a short biological half-life of 3–4 min in healthy adults. The rate
of allergic reaction was one per 333,000. The use of ICG for intraoperative perfusion angiography has been described previously22,23. ICG absorbs light in the NIR range of 790–805 nm, and
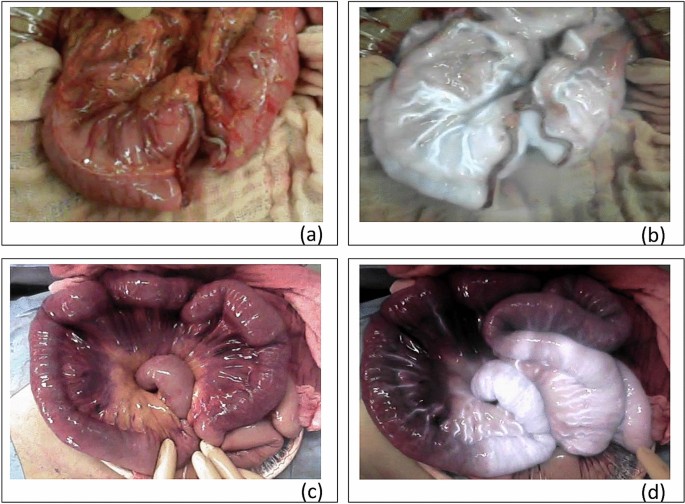
then reemits electromagnetic energy at 835 nm. This can be visualized by fluorescence due to the NIR irradiation13. The HyperEye Medical System (HEMS) provided by MIZUHO Medical (Tokyo,
Japan) was used at our institution. The HEMS super-sensitive optical sensor displays simultaneous fluorescence and color visible light images (Fig. 1). PROCEDURE Achieving hemostasis is the
main priority in hemodynamically unstable patients. NIR-ICG should be reserved for stable patients or during planned reoperation after emergency surgery. Intestinal resection was performed
in cases of grade ≥ 3 small bowel injury assessed using the American Association for the Surgery of Trauma (AAST) criteria. Colonic resection or stoma formation were performed in cases of
extensive colonic injury. After resection of the injured intestine, vascular perfusion at the stump was evaluated using NIR-ICG (Fig. 1a,b). Intestinal resection was performed for mesenteric
hematomas in cases of intestinal necrosis or vascular perfusion disorder. NIR-ICG was used to assess vascular perfusion where this was not clear, and in cases of intestinal strangulation by
the abdominal wall due to penetrating stab wounds. If there was a fluorescence delay, the intestine was resected (Fig. 1c,d). In the assessment of vascular perfusion, no resection was
performed for the normal flow type. In case of delayed inflow type, the area with impaired vascular perfusion compared to the surrounding bowel was resected. The delayed outflow type was not
measured in this study24. NIR-ICG was introduced into routine practice in 2013; prior to this date, the technique was used at the surgeon’s discretion. The dosage of ICG was 0.25 mg/kg. ICG
dye was injected and flushed through with 20 ml of saline, following which the ICG time was started and assessed using NIR fluorescence. Time to perfusion < 60 s was considered normal,
whereas a delay beyond 60 s or slower than the surrounding area suggested the presence of a vascular perfusion disorder requiring intestinal resection. STATISTICAL ANALYSIS All study
variables were compared between the NIR-ICG and non-NIR-ICG groups. Statistical analyses were performed using Mann–Whitney’s _U_ test for continuous variables or Fisher’s exact test for
categorical variables. A detailed analysis of cases with complications was performed, using Fisher’s exact test as well. Based on observed proportions in the study sub-group, 17 patients
guaranteed a power of 0.71 for 66% difference in a proportion of complications among two groups. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0.
(Armonk, NY: IBM Corp.). Statistical significance was set at p < 0.05. CONCLUSIONS The use of NIR-ICG tended to associate with the lower postoperative complications of intestinal and
mesenteric trauma. In addition, the use of NIR-ICG was associated with lower complications with statistical significance after intestinal resection. The NIR-ICG procedure is simple and quick
and is expected to be useful in intestinal and mesenteric trauma. Further studies are needed to confirm whether NIR-ICG can reduce complications, such as the AL rate in intestinal and
mesenteric injury. ABBREVIATIONS * HVI: Hollow viscus injury * AL: Anastomotic leakage * NIR: Near-infrared imaging * ICG: Indocyanine green * NIR-ICG: Near-infrared imaging using
indocyanine green * AAST: American Association for the Surgery of Trauma * CD grade: Clavien–Dindo grade * SSI: Surgical site infection * SBS: Short bowel syndrome REFERENCES * Swaid, F. _et
al._ Concomitant hollow viscus injuries in patients with blunt hepatic and splenic injuries: An analysis of a National Trauma Registry database. _Injury_ 45, 1409–1412 (2014). Article
Google Scholar * Abbasi, H. R. _et al._ Pattern of traumatic injuries and injury severity score in a major trauma center in Shiraz, Southern Iran. _Bull. Emerg Trauma._ 1, 81–85 (2013).
PubMed PubMed Central Google Scholar * Pekkari, P., Bylund, P. O., Lindgren, H. & Öman, M. Abdominal injuries in a low trauma volume hospital: A descriptive study from northern
Sweden. _Scand. J. Trauma Resusc. Emerg. Med._ 22, 48 (2014). Article Google Scholar * Arikanoglu, Z. _et al._ Factors affecting morbidity and mortality in hollow visceral injuries
following blunt abdominal trauma. _Clin. Ter._ 165, 23–26 (2014). CAS PubMed Google Scholar * Jha, N. K. _et al._ Characteristics of hollow viscus injury following blunt abdominal trauma;
a single centre experience from Eastern India. _Bull. Emerg. Trauma._ 2, 156–160 (2014). PubMed PubMed Central Google Scholar * Demetriades, D. _et al._ Penetrating colon injuries
requiring resection: Diversion or primary anastomosis? An AAST prospective multicenter study. _J. Trauma._ 50, 765–775 (2001). Article CAS Google Scholar * Curran, T. J. & Borzotta,
A. P. Complications of primary repair of colon injury: Literature review of 2,964 cases. _Am J Surg._ 177, 42–47 (1999). Article CAS Google Scholar * Inglin, R. A., Brügger, L. E.,
Candinas, D., Harrison, B. S. & Eberli, D. Effect of oxygen-producing suture material on hypoxic colonic anastomoses in an experimental model. _BJS Open._ 3, 872–881 (2019). Article CAS
Google Scholar * Vignali, A. _et al._ Altered microperfusion at the rectal stump is predictive for rectal anastomotic leak. _Dis. Colon. Rectum._ 43, 76–82 (2000). Article CAS Google
Scholar * Marquardt, C., Kalev, G. & Schiedeck, T. Intraoperative fluorescence angiography with indocyanine green: Retrospective evaluation and detailed analysis of our single-center
5-year experience focused on colorectal surgery. _Innov. Surg. Sci._ 5, 35–42 (2020). PubMed PubMed Central Google Scholar * Sheridan, W. G., Lowndes, R. H., Williams, G. T. & Young,
H. L. Determination of a critical level of tissue oxygenation in acute intestinal ischaemia. _Gut_ 33, 762–766 (1992). Article CAS Google Scholar * Karliczek, A. _et al._ Surgeons lack
predictive accuracy for anastomotic leakage in gastrointestinal surgery. _Int. J. Colorectal. Dis._ 24, 569–576 (2009). Article CAS Google Scholar * Ris, F. _et al._ Multicentre phase II
trial of near-infrared imaging in elective colorectal surgery. _Br. J. Surg._ 105, 1359–1367 (2018). Article CAS Google Scholar * McDermott, F. D. _et al._ Systematic review of
preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. _Br. J. Surg._ 102, 462–479 (2015). Article CAS Google Scholar * Watanabe, J. _et al._
Indocyanine green fluorescence imaging to reduce the risk of anastomotic leakage in laparoscopic low anterior resection for rectal cancer: A propensity score-matched cohort study. _Surg.
Endosc._ 34, 202–208 (2020). Article Google Scholar * Mirnezami, A. _et al._ Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: Systematic
review and meta-analysis. _Ann. Surg._ 253, 890–899 (2011). Article Google Scholar * Hammond, J., Lim, S., Wan, Y., Gao, X. & Patkar, A. The burden of gastrointestinal anastomotic
leaks: An evaluation of clinical and economic outcomes. _J. Gastrointest. Surg._ 18, 1176–1185 (2014). Article Google Scholar * Regina, D. L. _et al._ Financial impact of anastomotic
leakage in colorectal surgery. _J. Gastrointest. Surg._ 23, 580–586 (2019). Article Google Scholar * Flynn, D. N., Speck, R. M., Mahmoud, N. N., David, G. & Fleisher, L. A. The impact
of complications following open colectomy on hospital finances: A retrospective cohort study. _Perioper. Med._ 3, 1 (2014). Article Google Scholar * Schalamon, J., Mayr, J. M. &
Höllwarth, M. E. Mortality and economics in short bowel syndrome. _Best Pract. Res. Clin. Gastroenterol._ 17, 931–942 (2003). Article CAS Google Scholar * Anderson, D. J. _et al._
Strategies to prevent surgical site infections in acute care hospitals: 2014 update. _Infect. Control Hosp. Epidemiol._ 35, 605–627 (2014). Article Google Scholar * Cahill, R. A., Ris, F.
& Mortensen, N. J. Near-infrared laparoscopy for real-time intra-operative arterial and lymphatic perfusion imaging. _Colorectal. Dis._ 13(Suppl 7), 12–17 (2011). Article Google Scholar
* Ris, F. _et al._ Near infra-red laparoscopic assessment of the adequacy of blood perfusion of intestinal anastomosis: A video vignette. _Colorectal Dis._ 16, 646–647 (2014). Article CAS
Google Scholar * Yukaya, T. _et al._ Indocyanine green fluorescence angiography for quantitative evaluation of gastric tube perfusion in patients undergoing esophagectomy. _J. Am. Coll.
Surg._ 221, e37–e42 (2015). Article Google Scholar Download references ACKNOWLEDGEMENTS We thank all participants for attending and working through the study protocol. We would like to
thank Editage (www.editage.com) for English language editing. FUNDING This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit
sectors. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of Emergency Medicine, Yokohama City University Graduate School of Medicine, 4-57 Urafunecho, Minamiku, Yokohama, Japan
Keishi Yamaguchi, Takeru Abe, Kento Nakajima, Chikara Watanabe, Yusuke Kawamura, Tomoki Doi & Ichiro Takeuchi * Department of Surgery, Yokosuka Kyosai Hospital, 1-16 Yonegahama-dori,
Yokosuka, Japan Hirokazu Suwa, Yuta Minami, Kazunori Nojiri, Hidetaka Ono, Kenichi Yoshida & Hidenobu Masui Authors * Keishi Yamaguchi View author publications You can also search for
this author inPubMed Google Scholar * Takeru Abe View author publications You can also search for this author inPubMed Google Scholar * Kento Nakajima View author publications You can also
search for this author inPubMed Google Scholar * Chikara Watanabe View author publications You can also search for this author inPubMed Google Scholar * Yusuke Kawamura View author
publications You can also search for this author inPubMed Google Scholar * Hirokazu Suwa View author publications You can also search for this author inPubMed Google Scholar * Yuta Minami
View author publications You can also search for this author inPubMed Google Scholar * Kazunori Nojiri View author publications You can also search for this author inPubMed Google Scholar *
Hidetaka Ono View author publications You can also search for this author inPubMed Google Scholar * Kenichi Yoshida View author publications You can also search for this author inPubMed
Google Scholar * Hidenobu Masui View author publications You can also search for this author inPubMed Google Scholar * Tomoki Doi View author publications You can also search for this author
inPubMed Google Scholar * Ichiro Takeuchi View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS K.Y., T.A., H.S., Y.M., K.N., H.O., K.Y., H.M.,
and T.D. were involved in study design, data collection and data interpretation. K.Y., T.A., K.N., C.W., Y.K. and I.T. were involved in the data analysis. All authors critically revised the
report, commented on drafts of the manuscript, and approved the final report. CORRESPONDING AUTHOR Correspondence to Keishi Yamaguchi. ETHICS DECLARATIONS COMPETING INTERESTS The authors
declare no competing interests. ADDITIONAL INFORMATION PUBLISHER'S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional
affiliations. RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution
and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the
material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will
need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE
CITE THIS ARTICLE Yamaguchi, K., Abe, T., Nakajima, K. _et al._ Use of near-infrared imaging using indocyanine green associates with the lower incidence of postoperative complications for
intestinal and mesenteric injury. _Sci Rep_ 11, 23880 (2021). https://doi.org/10.1038/s41598-021-03361-1 Download citation * Received: 04 September 2021 * Accepted: 01 December 2021 *
Published: 13 December 2021 * DOI: https://doi.org/10.1038/s41598-021-03361-1 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable
link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative