15-min pedestrian distance life circle and sustainable community governance in chinese metropolitan cities: a diagnosis
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:

ABSTRACT Urban planning has shifted from “land-oriented” to “human-oriented” and metropolitan cities start to focus on 15-min life circle community planning during recent years. As multiple
dimensions of living service facilities are included, proactive supervision and real-time evaluation are essential in the governance and spatial planning of large cities, referring to urban
physical examination. This study proposes a community life circle diagnosis system based on multisource urban big data to evaluate the community public service facilities, in which the
performance of urban living service, in terms of fairness, accessibility, and diversity were assessed, and the services related to the health and emergency facilities apart from the daily
living service were investigated. Four representative Chinese megacities Beijing, Shanghai, Shenzhen, and Wuhan, were selected for the implementation and empirical analyses of the diagnosis
system, which were further compared regarding the existing community life circle facility service. Then, situations in Shanghai in 2011, 2016, and 2021 were longitudinally compared to verify
the influencing factors toward community life circle facilities. The results indicated that Shanghai has the highest quality of service of 15-min community life circle among the four
Chinese cities, followed by Shenzhen, Wuhan, and Beijing, according to the average coverage rate of citywide living service facilities. However, the municipal government in Shanghai still
needs to improve the investment in public resources in the suburbs, focusing on facilities related to elderly care, life security, and community travel. Findings of this study may assist
metropolitan development with policy and funding priorities, by using urban big data together with traditional empirical data (e.g. social-economic data, built environment, etc.) to diagnose
sustainable community development problems. SIMILAR CONTENT BEING VIEWED BY OTHERS MODELING WALKING ACCESSIBILITY TO URBAN PARKS USING GOOGLE MAPS CROWDSOURCING DATABASE IN THE HIGH-DENSITY
URBAN ENVIRONMENTS OF HONG KONG Article Open access 27 November 2023 THEORETICAL FRAMEWORK OF LIFE CIRCLES IN CHINESE SMALL TOWNS AND THE OPTIMIZATION OF SPATIAL LAYOUT FOR PUBLIC SERVICE
FACILITIES BASED ON RESIDENTS’ DISTANCE SENSITIVITY Article Open access 27 December 2024 A COMPREHENSIVE WALKABILITY EVALUATION SYSTEM FOR PROMOTING ENVIRONMENTAL BENEFITS Article Open
access 27 September 2023 INTRODUCTION The origin of the “life circle” can be traced back to “the third National Development Plan” initiated by Japan in the 1970s, which emphasizes the
spatial scope of community residents’ daily activities, such as shopping, leisure, commuting, and socializing by walking around their residences (Xiao et al., 2014). As the regular urban
walking speed is about 4–5 km per hour, the 15-min community can be interpreted as approximately 1 km walking distance. Consequently, a 15-min walking life circle covers 3–5 square
kilometers under ideal conditions, in which residents may access a variety of daily service facilities, such as education, health care, and leisure conveniently, thus satisfying the quality
and sustainability of lives. The core issue of community life circle construction is to rationally allocate a variety of public service facilities, with the layout directly affecting the
quality of urban residents’ lives. The early research mainly focused on the spatial accessibility of public service facilities, such as medical care, education, and parks (Weng et al.,
2019). Researchers have explored the impact of different types of facilities on social lives, such as the correlation between the accessibility of medical facilities and the healthy level of
residents (Van Herzele and Wiedemann, 2003), the correlation between the accessibility of food supermarkets and the incidence of obesity and other chronic diseases (Hare and Barcus, 2007),
the accessibility of schools and the career development of future generations (Pearce et al., 2007). A variety of measurements for accessibility of the facilities, e.g., container method
(Field et al., 2004), shortest distance method (Field et al., 2004), minimum travel cost (Smith et al., 2012), cumulative opportunity (Smith et al., 2012), kernel density (Boone et al.,
2009), gravity model (Boone et al., 2009), two-step mobile search (Luo and Wang, 2003), and so on, have been proposed accordingly. In fact, under the influence of the concept of spatial
justice, research interests have been increasing in the allocation of public service facilities in the community of socially vulnerable groups. Particularly, research on the spatial inequity
of public service facilities has become one of the hottest subjects in recent years, which refers to whether the accessibility of urban public service facilities is related to the
socioeconomic attributes or social demands of all residents (Talen, 1998). The common measurements include the Mann–Whitney _U_ test, ordered correlation analysis, analysis of variance,
bivariate spatial autocorrelation and regression analysis, etc. (Smoyer-Tomic et al., 2004). Areas with low socio-economic levels were found more likely to suffer from spatial inequity in
public service facility allocation. For example, Zenk et al. (Tan and Samsudin, 2017) analyzed community medical facilities and revealed spatial inequity in the distribution of breast
screening facilities in Chicago, where African–American citizens have relatively longer travel distances and bus travel time. Moreover, research on park crowding in Los Angeles revealed
significant differences in the quality of park services between blacks and whites, which occurs more in areas where blacks live (Zenk et al., 2006). Meanwhile, econometrics methods and
empirical models have been incorporated into the layout optimization and site selection of urban public service facilities (Bigman and Re Velle, 2010; Church and Velle, 1974; Langford et
al., 2008; Murray and Tong, 2007; Sister et al., 2010). Church and Velle (1974) proposed the maximal coverage model to obtain the optimal site selection scheme of facilities by maximizing
residential coverage under a given number of facilities. During the last 20 years, the focus has changed from the theoretical models on the location choice of public service facilities to
the simultaneous development of spatial optimization theory and practical applications. Langford et al. (2008) investigated the impact of population distribution on facilities in Cardiff,
UK, and put forward optimization strategies accordingly. Bigman and Re Velle (2010) studied the optimization model for the layout of public service facilities from the perspective of
consumer behavior patterns. For the location-allocation model, a commonly used model for layout optimization of public service facilities, Murray and Tong (2007) conducted a comprehensive
and systematic theoretical investigation of the spatial optimization model of public service facilities. Vora et al. (2015) proposed the optimal layout scheme of medical assistance
facilities in Western India using the location-allocation model. Although the objective in the configuration of almost all public service facilities is accessibility and availability, the
existing studies merely focused on one type or level of facilities, and seldom consider multiple types and levels of facilities comprehensively (Zhan et al., 2019). Meanwhile, the existent
situations were generally evaluated thus to propose optimization strategies and solutions, which unfortunately are devoid of longitudinal quantitative comparison in the time dimension to
evaluate the effectiveness of facility planning and construction (Zhan et al., 2019). This study proposes to evaluate urban development dynamics and promote high-quality and sustainable
urban development. A community life circle diagnosis was introduced for high-density megacities to carry out 15-min community life circle planning, analyzing the construction of community
life circle, and investigating the development trend of the community. Public service facility configuration was investigated as the core of community life circle planning. In addition to
the daily living service facilities, the study also includes health and emergency facilities and carries out a comprehensive assessment from the perspectives of both living services and
health and safety during COVID-19 pandemic prevention and control. Four Chinese megacities cities, namely Beijing, Shanghai, Shenzhen, and Wuhan, were selected as empirical examples in
spatial dimension to compare the construction quality of the community life circle. Meanwhile, Shanghai in 2011, 2016, and 2021 were selected as the investigating subjects for the
longitudinal comparison of the community life circle planning implementation results (Zhou, 2020). The remainder of the paper is structured as follows: section “Methods” presents the
framework of the evaluation system, as well as the empirical socioeconomical and community-built environmental data collection issues. Section “Empirical implementation and result analyses”
implements the diagnosis system first in the spatial dimension using Beijing, Shanghai, Shenzhen, and Wuhan, and then in the time dimension using the empirical situations of Shanghai in
2011, 2016, and 2021, respectively. Finally, conclusions and future research directions are provided in the section “Conclusions”. METHODS FRAMEWORK AND INDEXES OF EVALUATION SYSTEM With the
rapid development of urban science and technologies, the emergence of massive data enables to generate effective indexes to satisfy the living requirement of urban residents (Liu et al.,
2020; Zhan et al., 2018). The diagnosis system of the community life circle constructed adopted multisource urban data combined with the traditional statistical data (census population and
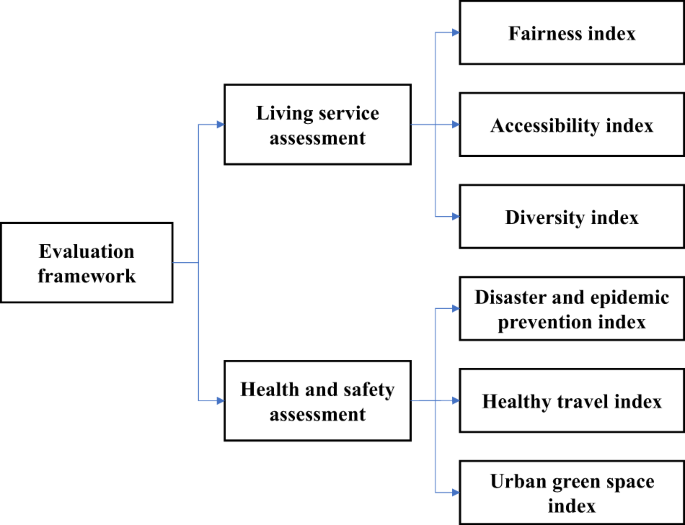
environment) and new big data (e.g., Point of Interest, POI and OpenStreetMap, OSM data) (Chen et al., 2020; Sun et al., 2016). The overall evaluation system consists of a living service
assessment, and a health & safety assessment, as presented in Fig. 1. The living service assessment was carried out from three aspects, including fairness, accessibility and diversity,
while the health and safety assessment mainly focused on disaster and epidemic prevention, healthy and sustainable travel and urban green space levels. LIVING SERVICE ASSESSMENT By sorting
out the relevant policy requirements of cities that have carried out life circle planning and summarizing the opinions from the selected experts, this study chose 16 living service
facilities in seven categories as the evaluation indexes, including education, culture, sports, administration, commerce, elderly care, and medical care. Basically, the fairness index mainly
assesses the existence of certain living service facilities, while accessibility and diversity indexes quantify the levels of service (QOS) based on certain principles, e.g. analytic
hierarchy process (AHP), Shannon–Wiener index. The specific measurement was conducted as follows: first, the pedestrian road networks for the life cycle were established within ArcGIS
software. Then, the service area of each residential area was determined with a buffer radius of 1000 m, to generate a 15-min community life circle. Finally, the distribution of living
service facilities within each community life circle was calculated and analyzed. FAIRNESS INDEX The fairness index was further divided into the coverage rate and the qualification rate. The
coverage rate reflects the proportion of the total number of residential neighborhood zones (RNZ) covered by living service facilities within a region, mainly measuring the construction
level of the community life circle. Here, RNZ refers to the areas with relatively concentrated residential buildings in cities, instead of an official administrative district. Taking the
city of Shanghai as an example, more than 27,000 sampling data were obtained from www.lianjia.com. The largest residential neighborhood zone of Shanghai Kangcheng in Xinzhuang Town has
12,238 households, with about 32,100 residents, while some small districts only have dozens of single-family villas or houses in suburban areas. In this study, RNZ _k_ is covered if
residents can reach type _i_ public service facility within 15-min walk (1000 m). The calculation formula is as follows: $$f\left( {C_{ki}} \right) = \left\{ {\begin{array}{*{20}{c}} 1 &
{\exists i \in I,{C_{ki}} \le 1000} \\ 0 & {\forall i \in I,{C_{ki}}{{{\mathrm{ > }}}}1000} \end{array}} \right.$$ (1) $$CR_{i} = \frac{{\mathop {\sum}\nolimits_{k = 1}^m {f\left(
{C_{ki}} \right)} }}{m}$$ (2) where _i_ is the facility type, _I_ is the collection of all facility types, _C__ki_ is the distance (m) between RNZ _k_ and facility type _i_, _m_ is the total
number of RNZs within the region, and _CR__i_ is the aggregated coverage rate of the public service facility type _i_. In addition to the coverage rate, the qualification rate considers the
daily demands of residents and the substitutability of various public service facilities, reflecting the construction completeness of the 15-min community life circle. Based on the survey
results of Ma et al. (2022), this study sets the relatively important and difficult-to-replace facilities as mandatory, while others may be substituted with each other as bonus ones.
Definitions of qualification criteria for the living service facilities are as follows: Education: Has kindergarten, primary school and middle school (all three)? Culture: Has community
cultural room, and one of either library or cultural activity center (at least one)? Sports: Has fitness center, playground and sports center (all three)? Administration: Has community
service center, and one of either district office or judicial office (at least one)? Commerce: Has food market and post office? Elderly care: Has elderly care facility? Medical care: Has
health center? ACCESSIBILITY INDEX As the number of facilities is also closely related to residents’ daily lives, the accessibility index was proposed to further measure the facilities in
the community life circle. The weight of each facility was determined with the AHP method (Golden et al., 1989). Fifty urban planning experts from Shanghai, Wuhan, Quanzhou, and Ningbo were
invited to rank and score the importance of various living service facilities, mainly consisting of experienced local planning policymakers and decision-makers. Based on the results,
education facilities were ranked as the most important in the community life circle, followed by commerce, medical care, sports, culture, and elderly care facilities, with the administration
facilities coming last. In addition to the experts, community residents from two megacities (Beijing, Shanghai) and four provinces (Guangdong, Jiangsu, Zhejiang, Hubei) were surveyed, to
rate the demand and importance of different facilities. 412 valid questionnaires were collected both online and offline, among which 26 persons in charge of neighborhood committees in
Shanghai were interviewed. According to the responses from the community residents, medical care facilities were ranked as the most important in daily life, followed by commerce, education,
sports, culture, elderly care, and administration facilities. High consistency was found between the survey results of community residents and expert opinions, as shown in Fig. 2. Only the
importance sequence of medical care and education facilities was changed, which may be due to the increased demand for neighborhood medical treatment during the COVID-19 epidemic. Therefore,
a judgment matrix of the pairwise relative importance of all categories of facilities was constructed based on the experts’ scorings as in Table 1. A similar calculation was carried out for
subclass facilities, with all results input into YAAHP, a decision analysis software based on AHP, to obtain the weight coefficients of living service facilities, as presented in Table 2.
Then, the accessibility index (_A__k_) of an RNZ _k_ is calculated as follows: $$A_{k} = \mathop {\sum}\limits_{i = 1}^n W_{i} \ast F_{ki}$$ (3) where _i_ is the facility type, _W__i_ is the
weight of facility _i_, _F__ki_ is the quantity index obtained after standardization covered by the life circle of RNZ _k_, and _n_ is the total number of facility types. DIVERSITY INDEX
When the fairness and accessibility indexes of two life circles are similar, the types of living service facilities owned by the two communities may be significantly different, although the
life circles with a balanced distribution of facilities tend to provide a higher level of service. Therefore, the facility diversity for each RNZ was measured by introducing Shannon–Wiener
index. The index was first used to calculate species diversity in the field of ecology, then extended to built environment areas (Frank and Pivo, 1994; Van Eggermond and Erath, 2016). The
calculation formula is as follows: $$H_{k} = - \mathop {\sum}\limits_{i = 1}^s {\frac{{n_{i}}}{N}} \ln \frac{{n_{i}}}{N}$$ (4) where _H__k_ is the diversity index of RNZ _k_, _i_ is the
facility type, _s_ is the number of facility type in the life circle, _n__i_ is the number of type _i_ facilities in the life circle, and _N_ is the total number of all facilities within the
life circle. HEALTH AND SAFETY ASSESSMENT During major public health events, e.g., COVID-19 epidemic prevention and control, “health” and “safety” become the primary goals of urban
residency. Therefore, the construction of disaster prevention, medical treatment, transportation, environment, and other related facilities in the community life circle were investigated.
DISASTER AND EPIDEMIC PREVENTION INDEX Community is the fundamental guarantee of urban society security. Starting from the resident demand when a community suffers from health and safety
emergencies, eight disaster and epidemic prevention facilities (affiliating to the three categories, named Disaster prevention, Community safety, and Life security) were proposed based on
the survey results (Ma et al., 2022). The accessibility of the facilities was introduced to evaluate the disaster and epidemic prevention capability of the community life circle. The weight
of each facility was determined through the AHP method, as presented in Table 3. Then, the disaster and epidemic prevention index in RNZ _k_ is calculated as follows: $$S_{k} = \mathop
{\sum}\limits_{i = 1}^n W_{i} \ast R_{ki}$$ (5) where _i_ is the facility type, _W__i_ is the weight of facility type _i_, _R__ki_ is the standardized quantity index of the _i_th type of
disaster and epidemic prevention facilities covered by the life circle of RNZ _k_, and _n_ is the total number of facility types. HEALTHY AND SUSTAINABLE TRAVEL INDEX Walking is the primary
mode of transportation within the life circle, while public transportation is more advocated for traveling between the communities. Access to a complete pedestrian network and a wide variety
of public transportation stations not only enable community residents to travel healthily but also provide more alternatives during safety emergencies (excluding epidemic events). These, in
turn, promote the community’s low carbon and sustainable capabilities, thus improving the health of the travel structure of daily travel and guaranteeing the safety of the community.
Therefore, considering the road network density and the number of bus stops covered within the life circle, the healthy and sustainable travel index for a residential area _k_ is calculated
as follows: $$T_{k} = D_{k} \ast P_{k}$$ (5) where _D__k_ is the road network density within the life circle of RNZ _k_, and _P__k_ is the number of public transportation stations covered by
the life circle of RNZ _k_ after standardization. URBAN GREEN SPACE INDEX As an essential part of urban infrastructure, green spaces not only improve the health performance of community
residents, enhancing the quality of the community environment but also improve the regional resilience to emergency events (Braubach et al., 2017). This study incorporated the evaluation of
green space into the diagnosis process of the community life circle, in which the area scope and accessibility significantly impact resident activities. The proposed index for a residential
area _k_ is calculated as follows: $$E_{k} = G_{k}/d_{k}$$ (6) where _G__k_ is the per capita public green space area within the life circle of RNZ _k_, and _d__k_ is the distance from
district _k_ to the nearest public green space, used to approximate the accessibility. STUDY AREA Four representative high-density megacities in China, namely Beijing (the Capital and the
largest city in north China), Shanghai (the economic center and the largest city in east China), Shenzhen (one of the most developed cities in south China), and Wuhan (capital of Hubei
province, and the largest city in central China) were selected as the investigation subjects, to implement the proposed diagnosis system on different empirical cases. Each city has a
permanent population of more than 10 million, representing the highest level of development in northern, eastern, southern and central China, respectively, as presented in Fig. 3a. Then,
Shanghai, the largest city in China, with 16 administrative districts, including seven central city areas and nine suburbs (Fig. 3b) was selected for a longitudinal comparison from the time
dimension. The changes and development of the community life circle from 2011 to 2021 were analyzed, thus assessing the implementation of the community life circle planning. DATA COLLECTION
AND CLEANSING The urban data used for the diagnosis system include residential, public service facilities, street networks, and other statistical data, among which the residential data were
derived from the Lianjia website (www.lianjia.com) and Amap (www.amap.com). The number of residential dataset records of Beijing, Shanghai, Shenzhen, and Wuhan in 2021 are 22,642, 27,466,
16,292, and 13,351, respectively after data cleanse, while those of Shanghai in 2016 and 2011 are 23,665 and 17,478. The public service facility datasets were derived from Amap POI. Overall
104,231, 119,571, 70,680, and 61,917 POI points of facilities in Beijing, Shanghai, Shenzhen, and Wuhan were collected for 2021 while the number of facility datasets for Shanghai in 2016 and
2011 are 95,324 and 55,379, respectively. The urban street network data was derived from the OSM map, on which some road sections were modified according to the existing conditions of each
city. The statistical data includes population and public green space areas. The population datasets were obtained from the census parcel data in each city, and the green space data were
derived from the official websites of urban landscaping bureaus and other relevant government sectors. EMPIRICAL IMPLEMENTATION AND RESULT ANALYSES SPATIAL DIMENSION EVALUATION LIVING
SERVICE ASSESSMENT RESULTS Table 4 presents the coverage rates for each category of living service facilities in Beijing, Shanghai, Shenzhen, and Wuhan, respectively. First, for the fairness
assessment, as the average coverage rates of living service facilities in the central areas of each city were calculated, which are significantly higher than those in the corresponding
suburbs. The four cities were ranked as Shanghai, Shenzhen, Wuhan, and Beijing, from high to low in terms of the coverage rate of living service facilities (82.4, 80.7, 78.1 and 75.1, as
presented in bold values). By each facility type, Beijing performs well in the medical care facility coverage rate, while Shanghai enjoys advantages in education, administration, and elderly
care facilities. Shenzhen has an outstanding culture, sports, and commerce facility coverage rate. The coverage rates of all facility types in Wuhan are at the middle level. One important
finding is that the coverage rate of elderly care facilities in Shenzhen is only 29%, far below that of the other three cities. This may be due to the reason that Shenzhen is an “immigrant”
city compared to the other cities, with rather younger residents. From the results of the qualification rate, the average quantity of qualification RNZs in central city areas of Beijing,
Shanghai, Shenzhen, and Wuhan are much higher than those of suburbs. In comparison, Shanghai has the highest average number of qualification indexes, attaining 6.5. When compared to the
suburbs, Shenzhen has the highest average number of 4.6. The average number of qualification indexes of all RNZs in Beijing, Shanghai, Shenzhen, and Wuhan cities are 4.9, 5.5, 5.1, and 5.3,
respectively. Figure 4 presents the spatial distribution of RNZs with different qualification indexes in the four cities. The RNZs with a high number of qualification indexes in Beijing,
Shanghai, and Wuhan are mainly concentrated in the central city areas. Additionally, a large number of RNZs were found with a high number of qualification indexes in the new suburban areas
of Shenzhen, where the overall distribution is relatively even. In terms of the proportion of the individual number of qualification indexes for the residential community, the proportion of
no one qualified (0) in Beijing is significantly higher than those in the other three cities. Most of these areas are distributed in the outer suburbs of the city. Shanghai accounted for the
highest proportion of full-qualified (7) by more than 30%, mainly distributed in the central city area. In terms of facility types, as presented in Fig. 5, both Shenzhen’s elderly care
facilities and Beijing’s culture facilities are low, which may require additional attention in future facility investment allocation. Next, for the accessibility assessment, Shanghai was
found with the highest overall accessibility index, as shown in Fig. 6a. Wuhan and Shenzhen have similar levels, and Beijing is with the lowest one. The accessibility of medical care
facilities in RNZs of Beijing is outstanding, while that of sports, administration, and elderly care facilities in Shanghai is relatively higher. A residential community in Shenzhen has the
advantage of the accessibilities of education, culture, and commerce facilities, while the accessibility of elderly care facilities is extremely lower than that of the other three cities.
Finally, for the diversity assessment, as shown in Fig. 6b, the facility types in central city areas of all four cities are more than those in the corresponding suburbs. Among them, Beijing
and Shanghai have the most significant difference in the types of facilities between central city areas and suburbs, with an average difference of four types. In contrast, Shenzhen has the
slightest difference of only 1.8. Overall, Shanghai performs the best, with an average of more than 13 types of facilities within the residential life circle citywide and more than 15 types
of facilities in the central city area. Beijing performs best in terms of the overall Shannon index, followed by Shanghai, Wuhan, and Shenzhen. HEALTH AND SAFETY ASSESSMENT RESULTS For the
disaster and epidemic prevention assessment, as shown in Fig. 7, Shenzhen has the best overall performance in disaster and epidemic prevention, followed by Shanghai and Wuhan, while Beijing
needs further efforts. By each facility type, Beijing has the advantage in the accessibility of community safety facilities. Shanghai has a higher level of disaster prevention facilities,
and Shenzhen has a relatively complete construction of life security facilities. Table 5 presents the results of the healthy travel assessment. Shanghai ranks first in the list with an
overall healthy travel index of 2.01 (in bold value), followed by Shenzhen. Wuhan and Beijing are on a similar level. The indexes in the central city areas of the four cities are higher than
that of the suburbs. Of the four cities, Shanghai has the largest difference in the indexes between the central city area and suburban (2.13), while that in Wuhan is the smallest (0.81), as
presented in bold values. The last one is urban green space assessment. As presented in Fig. 8, Shenzhen and Beijing are the top two cities benefiting from higher per capita public green
space. Although Wuhan has a higher per capita public green space than Shanghai citywide, it still ranks behind Shanghai on the overall urban green space index due to accessibility. For all
four cities, the indexes of the central city areas are higher than those of the suburbs. Shenzhen has the largest difference between the central city and suburban areas, while Shanghai and
Wuhan have comparable smaller differences. TIME DIMENSION EVALUATION LIVING SERVICE ASSESSMENT RESULTS As presented in Table 6, the average facility coverage rate in Shanghai has been
significantly improved during the last ten years (from 2011 to 2021), in which the improvement in suburban areas is slightly higher than that in central city areas. By the facility type,
education facilities only increase slightly. The coverage rate of primary and middle schools even decreased from 2011 to 2016 and then arose. Culture facilities have been improved
significantly, especially the cultural room, increasing from 7.2% to 44.3%. The coverage rates of sports and elderly care facilities, particularly the former one, increased significantly
from 2011 to 2016 and then steadily improved. The coverage rate of administration facilities remained stable, among which the coverage rate of the community center increased significantly.
The commerce and medical care facilities, which had already been with rather high coverage rates in 2011, did not change much during the last 10 years. On the qualification quantity, as
shown in Fig. 9a, the average qualification items in central city areas are significantly higher than those in suburban areas, and with comparable larger improvements in central city areas,
i.e., the difference between the central city and suburban areas increases. In terms of administrative division, Putuo District in the central city area and Baoshan District in the suburbs
increased the largest, while Chongming, Qingpu, and Jinshan Districts in the suburbs only increased slightly. By facility type, sports and culture facilities have improved the largest, as
presented in Fig. 9b. Sports facilities also have markedly improved from 2011 to 2016, while culture facilities have improved significantly from 2016 to 2021. From 2011 to 2016, facilities
for the elderly have significantly improved and remained stable since then. The qualification rates of education, commerce, and medical care facilities have remained steady, while
administration facilities have steadily improved over the years. In terms of diversity assessment, as presented in Fig. 10, the central city areas of Shanghai perform better than the
suburbs. All indexes are higher than the average values of the city, and the improvements in the central city areas are larger than that of the suburbs. Figure 10a shows that Putuo District
in the central city area and Baoshan District in the suburbs have the largest improvement. In contrast, Qingpu District and Chongming District in the suburbs have improved the least. The
number of facility types in Chongming District even decreased, which may be due to the reason that the improvement of facility construction did not catch up with the speed of residential
expansion. As presented in Fig. 10b, the Shannon Indexes of both Huangpu District in the central city area and Baoshan District in the suburban area have been improved significantly so that
the distribution of facility quantity has changed to a more balanced situation. Shannon indexes of four suburban districts, Chongming, Fengxian, Jiading, and Qingpu decreased during the
first five years (2011–2016). Then, the indexes in these areas keep increasing in the latter five years (2016–2021), which may benefit from the implementation of community life circle
planning in Shanghai in 2016. Regarding accessibility assessment, Fig. 11 presents the accessibility of living service facilities in Shanghai, which has steadily improved over the past
decade. Individual facility type, education, culture, and medical care facilities increased at a similar rate over the years. Sports facilities demonstrated the most remarkable improvement,
significantly higher in the first 5 years (2011–2016) than in the latter 5 years (2016–2021). On the contrary, the administration and commerce facilities showed comparable smaller
improvement during the first 5 years than in the latter five years. The accessibility of elderly care facilities improved the least, which remained almost unchanged during the last 5 years
(2016–2021). These to some extent reflected the emphasis on switching in facility allocation of Shanghai. To reveal the spatial distribution of the overall accessibility for the city, the
Bayesian Kriging interpolation analysis was carried out by taking each residential community as the measuring point (Gupta et al., 2017). Figure 12 shows the visualization results of the
spatial distribution of the overall accessibility index in Shanghai for 2011, 2016, and 2021, respectively. The accessibility index was categorized into six levels from lowest to highest
(using Natural Breaks). In 2011, all suburbs of Shanghai were with low indexes and only a small portion of central city areas were with high values. Since 2016, the overall accessibility of
facilities began to increase, and areas with high indexes started to appear in the “new center” of suburban administrative districts. The areas with high index in the central city also
expanded. By 2021, the low-value areas further shrunk, while the high-value areas continue to grow, and finally, the high-value areas started appearing in the suburbs. HEALTH AND SAFETY
ASSESSMENT RESULTS Figure 13 presents the empirical index values for disaster and epidemic prevention assessment, from which the improvement rate of Shanghai during the first 5 years
(2011–2016) was found less than that in the last 5 years (2016–2021). By each facility type, the improvement of community safety and life security facilities during the first 5 years was not
significant, much smaller than that in the last 5 years. The improvement of disaster prevention facilities was on the contrary. During the decade, the accessibility of disaster prevention
facilities improved the most, while the accessibility of life security facilities improved the least. From the perspective of spatial distribution, the trend is similar to the overall
accessibility index, as presented in Fig. 14. The high-value index areas existed in the central city areas in 2011 and then gradually spread outward. Table 7 presents the results of the
healthy travel assessment. The overall citywide travel index increased slightly from 1.82 to 2.01 during the decade. The indexes of central city areas are higher than suburban areas, and the
gaps in between increased over the years. From the perspective of spatial distribution, as presented in Fig. 15, the travel index in central city areas did not change significantly due to
intensive land use. With abundant land resources in the suburbs, new roads, metros, and transportation facilities substantially improved the convenience of community travel, and the
low-value areas decreased over the years (Sun and Ding, 2019; Zhong and Sun, 2022). In terms of urban green space assessment, as presented in Fig. 16, for each year the central city areas
perform better than the suburbs on average. The indexes of central city areas have improved more than the suburban areas during the past 10 years, with the difference in between increased.
In terms of administrative district, two suburb districts, Jiading and Minhang and two central city districts, Hongkou and Changning improved significantly during the decade, while the other
two suburb districts, Chongming and Baoshan only improved slightly. During the latter 5 years, the indexes of several suburb districts decreased, which may be related to the large-scale
expansion of suburban residential areas. CONCLUSIONS This study proposes a set of general diagnosis procedures for community life circles. Comprehensive analyses of the construction of the
life circles were carried out from both living services and health and safety. In terms of spatial dimension application, the latest assessments of Beijing, Shanghai, Shenzhen, and Wuhan in
2021 were implemented. The advantages and disadvantages of the facility configurations in each city were analyzed to assess the status quo of community life circle construction. The results
revealed that the four cities have different emphasizes on the construction of community life circles. Shanghai dominates in the construction level of administration, elderly care
facilities, and travel facilities. Shenzhen has achieved remarkable achievements in constructing culture, commerce, and safety-related facilities, while still lags when compared with the
other three cities in elderly care facilities. This might be mainly because the aging problem in Shenzhen is not as severe as in the other three cities.Footnote 1 Beijing has an outstanding
performance in urban green space assessment, which however needs more resource investments in community-level living service facilities. Most of the evaluation indexes in Wuhan are in the
middle level, which requires more investments in sports facilities, travel systems, and green community environment construction. The construction level of community life circles in the four
cities is more or less uneven in spatial development, manifested in that the indexes of life circles in the central city areas are better than those in the corresponding suburbs. Shenzhen
has the slightest difference between the central city and suburban areas among the four cities. The overall performance indexes indicate that Shanghai has the highest construction level of
15-min community life circle among the four cities, followed by Shenzhen, Wuhan, and Beijing. Results from the time dimension comparison in Shanghai (in 2011, 2016, and 2021) indicate that
the quality of community living service in central city areas has improved more than that of the suburbs during the past decade. Among all living community life circle services, sports
facilities have been improved the most, while elderly care facilities as the least, and other facilities steadily improved. As a society aging problem is becoming more severe in Shanghai
during recent years. More attention should be paid to the configuration of elderly care facilities. Meanwhile, the government needs to invest more public resources in the suburbs and
prioritize the resources towards facilities related to elderly care, life security, and community travel. By the empirical analyses and comparisons, planning problems for communities and
dwellings were revealed and quantitatively investigated through numerical analyses using massive multi-source data, providing technical support for government strategy stipulating and
decision-making. DATA AVAILABILITY Data sharing will be available upon reasonable request to the corresponding author by email directly. NOTES * Proportion of the population aged 60 and
above in Shenzhen, Shanghai, Beijing, and Wuhan is 5.36%, 23.38%, 19.64%, and 17.23%. Source: Bulletin of the Seventh National Census, 2021. REFERENCES * Bigman D, Re Velle C (2010) The
theory of welfare considerations in public facility location problems. Geogr Anal 10:229–240 Article Google Scholar * Boone CG, Buckley GL, Grove JM, Sister C (2009) Parks and people: an
environmental justice inquiry in Baltimore, Maryland. Ann Assoc Am Geogr 99:767–787 Article Google Scholar * Braubach M, Egorov A, Mudu P, Wolf T, Ward TC, Martuzzi M (2017) Effects of
urban green space on environmental health, equity and resilience. In: Kabisch N, Korn H, Stadler J, Bonn A (eds) Nature-based solutions to climate change adaptation in urban areas. Theory
and practice of urban sustainability transitions. Springer, Cham, pp. 187–205 Chapter Google Scholar * Chen F, Yin Z, Ye Y, Sun DJ (2020) Taxi hailing choice behavior and economic benefit
analysis of emission reduction based on multi-mode travel big data. Transp Policy 97:73–84 Article Google Scholar * Church R, Velle CR (1974) The maximal covering location problem. Pap Reg
Sci 32:101–118 Article Google Scholar * Field A, Witten K, Robinson E, Pledger M (2004) Who gets to what? Access to community resources in two New Zealand cities. Urban Policy Res
22(2):189–205 Article Google Scholar * Frank LD, Pivo G (1994) Impacts of mixed use and density on utilization of three modes of travel: single-occupant vehicle, transit, and walking.
Transp Res Rec 1466:44–52 Google Scholar * Golden BL, Wasil EA, Harker PT (1989) The analytic hierarchy process: applications and studies. Springer-Verlag, Berlin Book Google Scholar *
Gupta A, Kamble T, Machiwal D (2017) Comparison of ordinary and Bayesian kriging techniques in depicting rainfall variability in arid and semi-arid regions of north-west India. Environ Earth
Sci 76:512 Article ADS Google Scholar * Hare TS, Barcus HR (2007) Geographical accessibility and Kentucky’s heart-related hospital services. Appl Geogr 27:181–205 Article Google Scholar
* Langford M, Higgs G, Radcliffe J, White S (2008) Urban population distribution models and service accessibility estimation. Comput Environ Urban Syst 32:66–80 Article Google Scholar *
Liu J, Bi H, Wang M (2020) Using multi-source data to assess livability in Hong Kong at the community-based level: a combined subjective-objective approach. Geogr Sustain 1:284–294 Google
Scholar * Luo W, Wang F (2003) Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ Plan B 30:865–884 Article
Google Scholar * Ma W, Li L, Wang Y, He Q, Sun DJ (2022) Health examination evaluation system of community-life circle in high-density cities. J Tongji Univ (Nat Edn) 50(11):1627–1636
Google Scholar * Murray AT, Tong D (2007) Coverage optimization in continuous space facility siting. Int J Geogr Inf Sci 21(7):757–776 Article Google Scholar * Pearce J, Blakely T, Witten
K, Bartie P (2007) Neighborhood deprivation and access to fast-food retailing: a national study. Ame J Prev Med 32:375–382 Article Google Scholar * Sister C, Wolch J, Wilson J (2010) Got
green? Addressing environmental justice in park provision. GeoJournal 75:229–248 Article Google Scholar * Smith N, Hirsch D, Davis A (2012) Accessibility and capability: the minimum
transport needs and costs of rural households. J Transp Geogr 21:93–101 Article Google Scholar * Smoyer-Tomic KE, Hewko JN, Hodgson MJ (2004) Spatial accessibility and equity of
playgrounds in Edmonton, Canada. Can Geogr 48:287–302 Article Google Scholar * Sun DJ, Chen S, Zhang C, Shen S (2016) A bus route evaluation model based on GIS and super-efficient data
envelopment analysis. Transp Plan Technol 39(4):407–423 Article Google Scholar * Sun DJ, Ding X (2019) Spatiotemporal evolution of ridesourcing markets under the new restriction policy: a
case study in Shanghai. Transp Res Part A 130:227–239 Google Scholar * Talen E (1998) Visualizing fairness: equity maps for planners. J Am Plan Assoc 1:22–38 Article Google Scholar * Tan
PY, Samsudin R (2017) Effects of spatial scale on assessment of spatial equity of urban park provision. Landsc Urban Plan 158:139–154 Article Google Scholar * Van Eggermond M, Erath AL
(2016) Quantifying diversity: an assessment of diversity indices and an application to Singapore. FCL Mag Special Issue 4:30–37 Google Scholar * Van Herzele A, Wiedemann T (2003) A
monitoring tool for the provision of accessible and attractive urban green spaces. Landsc Urban Plan 63(2):109–126 Article Google Scholar * Vora KS, Koblinsky SA, Koblinsky MA (2015)
Predictors of maternal health services utilization by poor, rural women: a comparative study in Indian States of Gujarat and Tamil Nadu. J Health Popul Nutr 33:1–9 Article Google Scholar *
Weng M, Ding N, Li J, Jin X, Xiao H, He Z, Su S (2019) The 15-minute walkable neighborhoods: Measurement, social inequalities and implications for building healthy communities in urban
China. J Transp Health 13:259–273 Article Google Scholar * Xiao Z, Chai Y, Zhang Y (2014) Research progress of overseas life circle planning and practice. Planners 10:89–95. (in Chinese)
Google Scholar * Zenk SN, Tarlov E, Sun J (2006) Spatial equity in facilities providing low-or no-fee screening mammography in Chicago neighborhoods. J Urban Health 83:195–210 Article
PubMed PubMed Central Google Scholar * Zhan D, Kwan M, Zhang W, Fan J, Yu J, Dang Y (2018) Assessment and determinants of satisfaction with urban livability in China. Cities 79:92–101
Article Google Scholar * Zhan D, Zhang W, Chen L, Yu X, Dang Y (2019) Research progress and its enlightenment of urban public service facilities allocation. Prog Geogr 38:506–519. (in
Chinese) Google Scholar * Zhong S, Sun DJ (2022) Logic-driven traffic big data analytics: methodology and applications for planning. Springer Nature, p. 296 Book MATH Google Scholar *
Zhou X (2020) Assessing the distribution of public service facilities in unit planning based on the perspective of the 15-minute community-life circle: evidence from Huangpu district of
Shanghai. Urban Plan Forum 48(1):57–64 Google Scholar Download references ACKNOWLEDGEMENTS The research was funded in part by the National Nature Science Foundation of China [71971138,
52172319], and the National Social Science Foundation of China [22XJY030]. Part of the manuscript has been accepted and presented in the 102nd Transportation Research Board Annual Meeting,
Washington, DC in January 8–12, 2023. Any opinions, findings, and conclusions or recommendations expressed in this paper are those of the authors and do not necessarily reflect the views of
the sponsors. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * School of Design, Shanghai Jiao Tong University, No. 800 Dongchuan Road, Min-Hang District, 200240, Shanghai, China Wenjun Ma,
Ning Wang & Yuxi Li * College of Future Transportation, Chang’an University, Shangyuan Road, Weiyang District, 710021, Xi’an, China Daniel(Jian) Sun * Institute of National Security,
Shanghai Jiao Tong University, 200240, Shanghai, China Daniel(Jian) Sun Authors * Wenjun Ma View author publications You can also search for this author inPubMed Google Scholar * Ning Wang
View author publications You can also search for this author inPubMed Google Scholar * Yuxi Li View author publications You can also search for this author inPubMed Google Scholar *
Daniel(Jian) Sun View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS WM: Conceptualization, methodology, data curation, writing-original draft
preparation. NW: Writing-original draft preparation, Investigation. YL: Visualization, investigation, writing-original draft preparation. DJS: Supervision, writing-reviewing, and editing.
CORRESPONDING AUTHOR Correspondence to Daniel(Jian) Sun. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no competing interests. The authors confirm that the manuscript has been
read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed
in the manuscript has been approved by all of us. ETHICAL APPROVAL Ethical approval is not applicable for this article. INFORMED CONSENT There are no human subjects involved in this article
and informed consent is not applicable. ADDITIONAL INFORMATION PUBLISHER’S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional
affiliations. RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution
and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if
changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the
material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to
obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS
ARTICLE Ma, W., Wang, N., Li, Y. _et al._ 15-min pedestrian distance life circle and sustainable community governance in Chinese metropolitan cities: A diagnosis. _Humanit Soc Sci Commun_
10, 364 (2023). https://doi.org/10.1057/s41599-023-01812-w Download citation * Received: 27 December 2022 * Accepted: 26 May 2023 * Published: 29 June 2023 * DOI:
https://doi.org/10.1057/s41599-023-01812-w SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative