Identifying high-risk population of depression: association between metabolic syndrome and depression using a health checkup and claims database
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:

ABSTRACT Depression and metabolic syndrome (MetS) are correlated, leading to an increased healthcare burden and decreased productivity. We aimed to investigate the association between
MetS-related factors and depression using a health checkup and claims database. Individuals aged 18–75 years who underwent health examinations between 2014 and 2019 were enrolled in the
study. Among 76,277 participants, “ever” and “incident” antidepressant users exhibited worse metabolic profiles and were more likely to be prescribed hypnotics and anxiolytics than “never”
users. In a nested case–control study with a 1:10 ratio of incident users to controls, MetS was associated with incident antidepressant use (odds ratio, 1.53 [95% confidence interval
1.24–1.88]) adjusted for lifestyle information obtained from a self-administered questionnaire, medical history, and medications. Other metabolic traits also showed significant associations:
body mass index (1.04 [1.02–1.06]), abdominal circumference per 10 cm (1.17 [1.08–1.27]), high blood pressure (1.17 [1.00–1.37]), glucose intolerance (1.29 [1.05–1.58]), and dyslipidemia
(1.27 [1.08–1.51]). A bodyweight increase > 10 kg from age 20 years (1.46 [1.25–1.70]) was also significantly associated with incident antidepressant use. In conclusion, metabolic
abnormalities were associated with incident antidepressant use and can be useful in identifying populations at high risk of depression. SIMILAR CONTENT BEING VIEWED BY OTHERS INCREASED ODDS
OF METABOLIC SYNDROME AMONG ADULTS WITH DEPRESSIVE SYMPTOMS OR ANTIDEPRESSANT USE Article Open access 27 February 2025 ASSOCIATION BETWEEN DEPRESSION AND DIABETES AMONG AMERICAN ADULTS USING
NHANES DATA FROM 2005 TO 2020 Article Open access 12 November 2024 EXPLORING THE RELATIONSHIP BETWEEN THE URIC ACID TO HIGH-DENSITY LIPOPROTEIN CHOLESTEROL RATIO AND DEPRESSION: A
CROSS-SECTIONAL STUDY FROM NHANES Article Open access 30 December 2024 INTRODUCTION Depression is one of the most common mental illnesses affecting working-age adults and is a major public
health problem worldwide1. Depression is associated with increased mortality in the general population and among persons with comorbidities2,3,4,5. A growing body of evidence demonstrates
that depression is associated with an increased risk of physical disease, including diabetes mellitus6,7 and cardiovascular disease (CVD)2,8,9,10. Furthermore, mental disorders including
depression account for approximately 20–50% of disability benefits across the Organisation for Economic Co-operation and Development countries11 and have been found to significantly reduce
the ability of people to work by increasing other disabilities, including physical ailments12,13. Thus, depression not only has the potential to increase net healthcare costs for the
treatment of various physical illnesses in addition to depression, but can also cause presenteeism and absenteeism, which potentially lead to lost productive time in the workplace14,15.
Various comorbidities, such as cancer, stroke, and diabetes mellitus, are associated with the incidence of depression16,17,18. A systematic review revealed that depression is two to three
times more likely to occur in people with multimorbidity than in those without multimorbidity or those with no chronic physical condition. Metabolic syndrome (MetS) is a pre-symptomatic
state and is defined as a combination of abdominal or visceral obesity, hypertension, dyslipidemia, and glucose dysregulation, and it has a diagnostic significance in predicting subsequent
coronary artery disease, metabolic diseases, and certain cancers19,20. Previous studies showed that even MetS is associated with the development of depression21,22. However, few longitudinal
studies have demonstrated the association between MetS and depression, and knowledge regarding the association between lifestyle and depression remains limited. In Japan, universal health
screening and health guidance were initiated in the early 2000s with the main objective of detecting high-risk populations for CVD23. Since then, the word “_metabo_” has been coined in
Japan, and this health checkup has become more widespread and promoted. However, one study showed that the effectiveness of prevention of CVD and improvement of anthropometric metrics was
limited24. Although this is different from the original purpose of this health checkup, if the data from this checkup can be used to show an association between MetS and depression, it may
be possible to identify people at high risk of developing depression and add new significance to universal health screening and health guidance. Therefore, this study aimed to examine the
association between MetS-related factors and the development of depression after adjustment for various factors such as medication, prior hospitalization, and lifestyle. We used health
insurance claims and health checkup data of corporate insurance beneficiaries, who are representative of the major workforce in Japan. These data covered medical costs, hospitalizations,
disease codes, and prescription medicines, allowing us to adjust for comprehensive factors related to the medical interventions received by study participants. RESULTS BASELINE
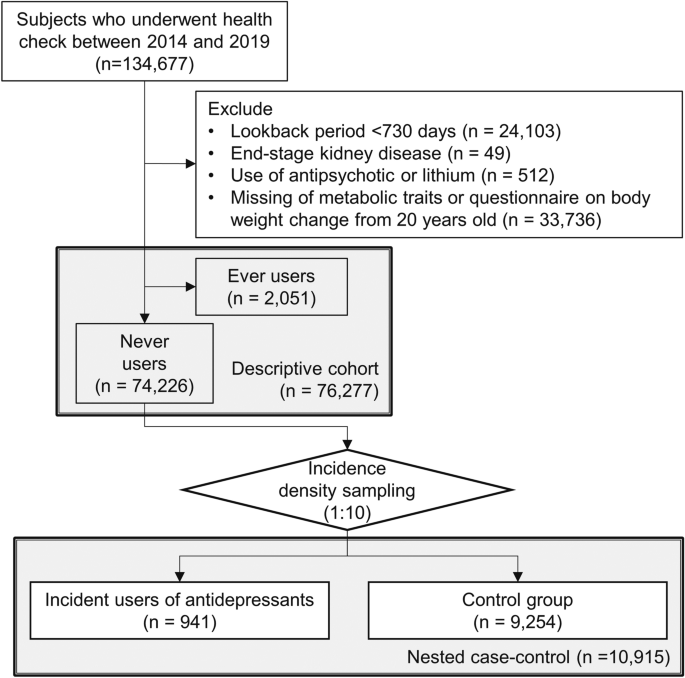
CHARACTERISTICS OF THE OVERALL STUDY POPULATION Individuals aged 18–75 years who underwent health examinations between April 1, 2014, and March 31, 2019, were enrolled in the study. The flow
diagram shows the study population and overall study design (Fig. 1). Participants with the following characteristics were excluded: a lookback period < 730 days (n = 33,299); end-stage
kidney disease (n = 49); use of second generation antipsychotics or lithium (n = 512); missing information on the following metabolic traits: body mass index (BMI), blood pressure (BP), or
abdominal circumference (AC); missing laboratory data on hemoglobin A1c (HbA1c), fasting blood glucose, triglycerides (TG), high-density lipoprotein cholesterol (HDL-c), or low-density
lipoprotein cholesterol (LDL-c); or missing questionnaire on bodyweight change from age 20 (n = 33,736). In the descriptive cohort, 76,277 individuals were eligible for the study, including
2051 individuals who had ever used or were currently using antidepressants, 74,226 who had never used antidepressants, and 941 incident users of antidepressants after baseline. The baseline
characteristics of “ever”, “never”, and “incident” users of antidepressants in the descriptive cohort are shown in Table 1. Ever users had a higher proportion of diabetes mellitus and
dyslipidemia cases than the other users. Ever and incident users had a high proportion of MetS cases. Questionnaires on lifestyle revealed that never users were less likely to experience
bodyweight increase and poor sleep and more likely to be physically active. Late supper, skipping breakfast, and eating speed were not clinically different across the groups. The
questionnaire on bodyweight change showed that ever and incident users were more likely to experience bodyweight increase from the age of 20. Regarding alcohol-drinking habits, never users
had a lower proportion of occasional or daily drinkers than the others. Regarding medication, incident users were more likely to be prescribed hypnotics and analgesics than never users;
furthermore, ever users were considerably more likely to be prescribed hypnotics than incident users (Fig. 2a). Regarding hospitalization records, ever and incident users were more likely to
be hospitalized, especially cancer-related hospitalization (Fig. 2b). NESTED CASE–CONTROL STUDY TO EXAMINE THE FACTORS ASSOCIATED WITH INCIDENT ANTIDEPRESSANT USE After excluding ever users
of antidepressants from the descriptive cohort, we performed a nested case–control study to examine the factors associated with incident antidepressant use. The nested case–control design,
also known as risk-set sampling, is a type of study design that identifies controls from a group of people who are “at risk” at the index date of the case25. Herein, we defined the day of
the first filling of an antidepressant prescription as the index date. For each case, up to 10 controls were selected, and they were selected from subjects of the same sex and age ± 3 years;
hence, we finally analyzed the data of 10,915 individuals, including 941 incident users and 9254 controls. The baseline characteristics are compared in Table 2. Incident users had a higher
proportion of MetS cases and hypnotic and analgesic users, and they were more likely to experience body weight increase from age 20 and any hospitalization and cancer-related
hospitalizations prior to the index date. Table 3 shows the results of both univariable and multivariable conditional logistic regression analyses to examine associations with incident
antidepressant use (case). MetS was significantly associated with the incident antidepressant use in Model 3 (adjusted odds ratio, 1.53 [95% confidence interval 1.24–1.88]). Lifestyle,
eating speed, poor sleep, and drinking habits were significantly associated with the outcome. Hospitalization due to cancer and use of hypnotics and anxiolytics were also significantly
associated with the outcome. Regarding other metabolic traits, BMI, AC, high BP, glucose intolerance, dyslipidemia, a > 10 kg increase in bodyweight from age 20, and the number of
metabolic components were also significantly associated with antidepressant initiation (Table 4). Here, the number of metabolic components was defined as the number of cases with high BP,
glucose intolerance, and dyslipidemia. As a sensitivity analysis, the same analysis as in Tables 2 and 3 was performed for the lookback period of 1 year; data from 14,337 individuals,
including 1330 affected individuals and 13,307 controls, were analyzed (Supplementary Fig. 1). Similar results were obtained in Supplementary Table 1 and 2. DISCUSSION This study clearly
demonstrated that MetS was associated with the incident use of antidepressants after adjustment for various medical and lifestyle factors using large-scale real-world data from health
insurance claims and health checkups in Japan. The major finding of the present study was that MetS, other metabolic abnormalities, and pre-symptomatic conditions, including BMI, AC, high
BP, glucose intolerance, and dyslipidemia, were associated with antidepressant initiation. We also showed that bodyweight increase of > 10 kg from the age of 20 years was associated with
the incident use of antidepressants. MetS and its components were associated with the incident use of antidepressants independent of lifestyle, cancer-related or CVD-related
hospitalizations, and medications. We also demonstrated a dose–response association between the number of metabolic components and incident antidepressant use. These findings were of
particular interest in that the sum of pre-symptomatic conditions alone was associated with the development of depression despite the absence of a need for disability acceptance or problems
with life dysfunction. This study allowed us to add more significance to health checkups: for screening individuals at high risk of depression. In Japan, a survey showed that the lifetime
prevalence and 12-month prevalence of major depressive disorder were 6.1% and 2.2%, respectively, and that the proportion of individuals receiving any type of treatment was 38.7%, which was
lower than that in many other high-income countries26. The survey found that over 70% of people have moderate or severe depression, yet the low percentage receiving appropriate treatment is
problematic. Now that this study showed that MetS is a risk factor for depression, we expect that health checkups and specified health guidance will have a new role as screening sessions for
depression and will increase public awareness of the opportunity for early consultation and early appropriate treatment for depression. The pathways from MetS to depression could be
biological or social27, a phenomenon that can be explained by the physiological consequences of obesity, including higher inflammation28,29 and the psychological/social consequences of MetS
or obesity. However, most of the health-related behaviors assessed by the questionnaire, such as exercise habits, late supper, skipping breakfast, and smoking, were not significantly
different between the cases and controls. Notably, information on physical activity or exercise habits was collected using self-administered questionnaires rather than quantitative methods.
More detailed research is required to investigate physical activity and exercise habits more quantitatively and accurately through a quantitative physical activity using biometric sensors
and detailed questionnaires on exercise habits. Regarding psychosocial factors, physical and mental stress can be common causes of MetS and depression. The study subjects were corporate
insurance beneficiaries comprising corporate employees and their dependents, and mental stress is potentially caused by the work itself, human relationships in the workplace, and family
issues in this population. Physical stress may be caused by shift work. These not only trigger depression, but can also result in obesity and MetS through overeating, sleep disorders, and
effects on various metabolic systems. However, this study did not include information such as work shifts and work-related stress, and further studies are required to identify modifiable
factors and identify solutions to overcome both health issues. We also observed interesting findings regarding lifestyle. First, we found that alcohol consumption is potentially protective
against depression. Several previous studies have shown consistent results regarding the protective effect of alcohol against depression30,31,32,33,34. Although our results did not show a
clear benefit of daily physical activity and modifiable lifestyle factors including sleep and exercise habits as potential candidates for intervention in depression and MetS. Daily exercise
habits are particularly suitable lifestyle interventions, as a large body of evidence demonstrates the effectiveness of exercise on depression and sleep disorders35,36,37,38. Regarding
prescription medicine, the use of hypnotics, anxiolytics, and NSAIDs at baseline was associated with incident antidepressant use. Studies have shown that insomnia is associated with
depression and anxiety disorders39,40. However, depression is often underdiagnosed in primary-care settings or for older patients41, and such medications might have been prescribed as
supportive care for patients with symptoms and complaints related to depression but not formally diagnosed. Hence, individuals with underdiagnosed and undertreated depression may be hidden
among those who have been prescribed these drugs. Finally, a history of hospitalization for malignant diseases was also associated with incident antidepressant use. However, the association
was attenuated after adjusting for medication information. This may be due to the mediation effects of anxiety and insomnia on the association. Previous studies have demonstrated that
anxiety, depression, and insomnia are associated with cancer as well as with increased adverse outcomes, including mortality and psychosocial problems in cancer survivors42,43,44,45. The
present study reaffirms the importance of psychological care for those who experience cancer-related hospitalization. This study had certain limitations. First, the present study was
observational and did not demonstrate any causality. However, our results revealed various medical and lifestyle factors associated with depression, which we believe provide valuable
insights into workplace mental and physical health. Second, we classified depression based on specific, prescribed classes of antidepressants, that is, selective serotonin reuptake
inhibitors (SSRIs), serotonin-noradrenalin reuptake inhibitors (SNRIs), or noradrenergic and specific serotonin antidepressants (NaSSAs), thus potentially leading to misclassification bias
since those who were treated with other classes of medication or those who had not been treated with medication were not diagnosed with depression. This type of misclassification is
unavoidable in large-scale database studies. However, the main purpose of this study was to explore and generate hypotheses for future research. Therefore, sufficient findings have been
generated from this analysis. Third, there was a concern regarding selection bias. Those who were taking sick leave due to depression might not have undergone health checkups in the
workplace. However, in our country, the number of individuals who undergo health checkups is high in the working generations. Finally, most of the lifestyle information was derived from
self-administered questionnaires, thus potentially undermining accuracy and objectivity. Furthermore, recall bias may have existed when filling out the questionnaire. We may consider using
activity monitoring46, such as gyrometers, to gain objective personal activity information in future studies. In conclusion, MetS and other metabolic abnormalities were associated with
incident antidepressant use in working-age individuals. This study also allowed us to add more significance to health checkups: for screening individuals at high risk of depression.
Lifestyle intervention could be the subsequent step in reducing both mental and physical burdens among individuals in their prime. METHODS DATA SOURCE AND ETHICAL ISSUES The data source
comprised anonymized, processed receipt information and medical checkup data provided by health insurance associations in Japan contracted with PREVENT Co., Ltd, stored at the company. The
present study analyzed data from the administrative claims-based database that included information on 134,677 individuals who underwent health examinations at least once and were under
health insurance coverage between April, 2014 and March, 2019, targeted at corporate employees and their dependents in Japan. All data was extracted and processed on November 17, 2020. We
conducted this study in accordance with the guidelines of the Declaration of Helsinki. The institutional ethics committee of Nagoya University Graduate School of Medicine formally approved
this study (Approval No. 2020-0142). The Ethical Review Committee for Observational Research is an officially approved and registered organization (No. 15000226). Since the study data were
provided anonymously, and the study participants did not receive any intervention, informed consent for study participation was waived by ethics committee of Nagoya University Graduate
School of Medicine. DEFINITIONS We obtained the following information from checkup data: sex, age, BMI, BP, and AC data; laboratory data on HbA1c, fasting blood glucose, TG, HDL-c, and
LDL-c; smoking and alcohol habits; and lifestyle and behavior, including weight changes, exercise habits, physical activity, walking speed, eating speed and habits, and poor sleep. Blood
tests and physical measurements such as BMI, BP, and AC were performed at the nearest local clinic, hospital, or health screening center for each subject, using standard procedures. A
habitual cigarette smoker was defined as a person who smoked a total of over 100 cigarettes or for over six months and has smoked in the last month. Exercise habits were defined as
exercising to sweat lightly for > 30 min per session, twice weekly, for over a year. Physical activity was defined as walking or performing an equivalent amount of physical activity for
> 1 h per day. Fast walking speed was defined as faster speed than that of almost the same age and of the same gender. Eating speed was categorized into the following three categories:
“quicker” than others, “normal,” and “late.” Late supper was defined as eating supper 2 h before bedtime more than three times a week. Skipping breakfast was defined as skipping breakfast
more than three times a week. Bodyweight change was defined as a > 10 kg increase in body weight from the age of 20 years. We defined the following medicines or their combination as
antidepressants: SSRI, SNRI, and NaSSA. We did not include other types of classical antidepressants, including tricyclic or tetracyclic antidepressants, or serotonin antagonists and reuptake
inhibitors, since they have been used for purposes other than depression treatment. We defined “ever” users as individuals whose last antidepressant prescription filling was earlier than 30
days after the baseline date and “never” users as those who had never been prescribed an antidepressant within 30 days after the baseline date (Fig. 3). “Incident” users were defined as
individuals who had not been prescribed any antidepressants for at least the past 2 years (730 days) and who were initiated on antidepressants > 30 days after the baseline date. In a
prior study, the lookback period was set as 1 year47. However, the study population comprised youths who were 5 to 20 years of age. Considering the lifelong recurrence of major depressive
disorder, we set the lookback period as 2 years48. For sensitivity analysis, we set the lookback period as 1 year and performed the same analysis. Additionally, we obtained baseline data on
medication history other than antidepressants, disease name, hospitalization, and procedure from the claims data prior to 30 days after the baseline. A positive medication history was
defined as at least one prescription filling during the study period. Data on antihypertensive agents, antidiabetic agents, statins, hypnotics, and NSAIDs were collected using the World
Health Organization anatomical therapeutic chemical classification codes (Supplementary Table 2). Detailed information on drug code combinations representing these drugs is available on
GitHub (https://github.com/PREVENT-Inc/MyscopeMasterList/tree/master/nagoya-u/medical_conditions_and_depression). Hospitalization information was also obtained from claims data prior to 30
days after the baseline date. Hospitalizations due to specific causes were defined using a combination of the International Statistical Classification of Diseases and Related Health Problems
(ICD)-10 codes in the hospitalization information of medical claims data. Herein, we classified hospitalizations into the following categories: any cause, CVD, congestive heart failure,
cancer, and psychotic disorders. CVD-related hospitalization was defined as having any of the following diseases: acute myocardial infarction, congestive heart failure, and cerebrovascular
disease. The combinations of ICD-10 codes have been described in a previous study by Quan et al.49 Hospitalizations due to mental disorders were classified based on the ICD-10 classification
of mental and behavioral disorders50. STATISTICAL ANALYSIS For between-group comparisons, categorical variables are expressed as numbers and percentages, and continuous variables as the
median (interquartile range) or mean (standard deviation). In the nested case–control study, a between-group comparison was performed in a fashion similar to the comparison of the overall
study participants. Univariable and multivariable conditional logistic regression was used to examine the factors associated with the incident prescription of antidepressants. Covariates
included age; sex; smoking and drinking habits; physical activity; poor sleep; the use of hypnotics, anxiolytics, and NSAIDs; and hospitalizations due to CVD and cancer. Hospitalization
records were utilized in a time-updated manner, implying that hospitalization records were collected not only from baseline but also from data prior to the index dates. Two-sided statistical
significance was set at P < 0.05. All analyses were performed using Stata version 17.0 software (StataCorp, TX, USA). DATA AVAILABILITY The data used in this study is the property of
PREVENT Co., Ltd. and the purpose of use is restricted by PREVENT’s policy on data utilization. The data used in this study was also used under contract and is not available to the public.
Inquiries about the data can be made via GoogleForm [https://forms.gle/iWbhLjEx157dkXZB9], and can available after a license agreement is signed. REFERENCES * James, S. L. _et al._ Global,
regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global
Burden of Disease Study 2017. _Lancet_ 392, 1789–1858 (2018). Article Google Scholar * Meng, R. _et al._ Association of depression with all-cause and cardiovascular disease mortality
among adults in China. _JAMA Netw. Open_ 3, e1921043 (2020). Article PubMed PubMed Central Google Scholar * Gilman, S. E. _et al._ Depression and mortality in a longitudinal study:
1952–2011. _CMAJ_ 189, E1304–E1310 (2017). Article PubMed PubMed Central Google Scholar * Carney, R. M. & Freedland, K. E. Depression, mortality, and medical morbidity in patients
with coronary heart disease. _Biol. Psychiatry_ 54, 241–247 (2003). Article PubMed Google Scholar * Katon, W. J. _et al._ The association of comorbid depression with mortality in patients
with type 2 diabetes. _Diabetes Care_ 28, 2668–2672 (2005). Article PubMed Google Scholar * Nouwen, A. _et al._ Longitudinal associations between depression and diabetes complications: A
systematic review and meta-analysis. _Diabet. Med._ 36, 1562–1572 (2019). Article CAS PubMed Google Scholar * Mezuk, B., Eaton, W. W., Albrecht, S. & Golden, S. H. Depression and
type 2 diabetes over the lifespan: A meta-analysis. _Diabetes Care_ 31, 2383–2390 (2008). Article PubMed PubMed Central Google Scholar * Musselman, D. L., Evans, D. L. & Nemeroff, C.
B. The relationship of depression to cardiovascular disease: Epidemiology, biology, and treatment. _Arch. Gen. Psychiatry_ 55, 580–592 (1998). Article CAS PubMed Google Scholar * Hare,
D. L., Toukhsati, S. R., Johansson, P. & Jaarsma, T. Depression and cardiovascular disease: A clinical review. _Eur. Heart J._ 35, 1365–1372 (2014). Article PubMed Google Scholar *
Zhang, Y., Chen, Y. & Ma, L. Depression and cardiovascular disease in elderly: Current understanding. _J. Clin. Neurosci._ 47, 1–5 (2018). Article PubMed Google Scholar * Organisation
for Economic Co-operation and Development. Sickness, Disability and Work: Breaking the Barriers. _OECD_
https://www.oecd.org/publications/sickness-disability-and-work-breaking-the-barriers-9789264088856-en.htm. https://doi.org/10.1787/9789264088856-EN (2010) * Savikko, A., Alexanderson, K.
& Hensing, G. Do mental health problems increase sickness absence due to other due to other diseases?. _Soc. Psychiatry Psychiatr. Epidemiol._ 36, 310–316 (2001). Article CAS PubMed
Google Scholar * Kessler, R. C., Ormel, J., Demler, O. & Stang, P. E. Comorbid mental disorders account for the role impairment of commonly occurring chronic physical disorders: Results
from the National Comorbidity Survey. _J. Occup. Environ. Med._ 45, 1257–1266 (2003). Article PubMed Google Scholar * Stewart, W. F., Ricci, J. A., Chee, E., Hahn, S. R. &
Morganstein, D. Cost of lost productive work time among US workers with depression. _J. Am. Med. Assoc._ 289, 3135–3144 (2003). Article Google Scholar * Kessler, R. C. The costs of
depression. _Psychiatr. Clin. N. Am._ 35, 1–14 (2012). Article Google Scholar * Robinson, R. G. Poststroke depression: Prevalence, diagnosis, treatment, and disease progression. _Biol.
Psychiatry._ 54, 376–387 (2003). Article PubMed Google Scholar * Krebber, A. M. H. _et al._ Prevalence of depression in cancer patients: A meta-analysis of diagnostic interviews and
self-report instruments. _Psychooncology_ 23, 121–130 (2014). Article CAS PubMed Google Scholar * Campayo, A., Gómez-Biel, C. H. & Lobo, A. Diabetes and depression. _Curr Psychiatry
Rep._ 13, 26–30 (2011). Article PubMed Google Scholar * Eckel, R. H., Grundy, S. M. & Zimmet, P. Z. The metabolic syndrome. _Lancet_ 365, 1415–1428 (2005). Article CAS PubMed
Google Scholar * Grundy, S. M. _et al._ Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement.
_Circulation_ 112, 2735–2752 (2005). Article PubMed Google Scholar * Marazziti, D., Rutigliano, G., Baroni, S., Landi, P. & Dell’Osso, L. Metabolic syndrome and major depression. _CNS
Spectr._ 19, 293–304 (2014). Article PubMed Google Scholar * Pan, A. _et al._ Bidirectional association between depression and metabolic syndrome: A systematic review and meta-analysis
of epidemiological studies. _Diabetes Care_ 35, 1171–1180 (2012). Article PubMed PubMed Central Google Scholar * Takahara, M. & Shimomura, I. Metabolic syndrome and lifestyle
modification. _Rev. Endocr. Metab. Disord._ 15, 317–327 (2014). Article CAS PubMed Google Scholar * Fukuma, S., Iizuka, T., Ikenoue, T. & Tsugawa, Y. Association of the National
Health Guidance Intervention for Obesity and Cardiovascular Risks with Health Outcomes among Japanese Men. _JAMA Intern. Med._ 180, 1630–1637 (2020). Article PubMed PubMed Central Google
Scholar * Langholz, B. & Goldstein, L. Risk set sampling in epidemiologic cohort studies. _Stat. Sci._ 11, 35–53 (1996). Google Scholar * Ishikawa, H., Kawakami, N. & Kessler, R.
C. Lifetime and 12-month prevalence, severity and unmet need for treatment of common mental disorders in Japan: Results from the final dataset of World Mental Health Japan Survey.
_Epidemiol. Psychiatr. Sci._ 25, 217 (2016). Article CAS PubMed Google Scholar * Casanova, F. _et al._ Higher adiposity and mental health: Causal inference using Mendelian randomization.
_Hum. Mol. Genet._ 30, 2371–2382 (2021). Article CAS PubMed PubMed Central Google Scholar * Miller, A. H. & Raison, C. L. The role of inflammation in depression: From evolutionary
imperative to modern treatment target. _Nat. Rev. Immunol._ 16, 22–34 (2016). Article CAS PubMed PubMed Central Google Scholar * Lawlor, D. A., Smith, G. D. & Ebrahim, S.
Association of insulin resistance with depression: Cross sectional findings from the British women’s heart and health study. _BMJ_ 327, 1383–1384 (2003). Article PubMed PubMed Central
Google Scholar * García-Esquinas, E. _et al._ Moderate alcohol drinking is not associated with risk of depression in older adults. _Sci. Rep._ 8, 11512 (2018). Article ADS PubMed PubMed
Central Google Scholar * Cheng, H. G., Chen, S., McBride, O. & Phillips, M. R. Prospective relationship of depressive symptoms, drinking, and tobacco smoking among middle-aged and
elderly community-dwelling adults: Results from the China Health and Retirement Longitudinal Study (CHARLS). _J. Aff. Disord._ 195, 136–143 (2016). Article Google Scholar * Paulson, D. _et
al._ The relationship between moderate alcohol consumption, depressive symptomatology, and C-reactive protein: The Health and Retirement Study. _Int. J. Geriatr. Psychiatry_ 33, 316–324
(2018). Article PubMed Google Scholar * Gea, A. _et al._ Alcohol intake, wine consumption and the development of depression: The PREDIMED study. _BMC Med._ 11, 192 (2013). Article PubMed
PubMed Central Google Scholar * Bellos, S. _et al._ Longitudinal association between different levels of alcohol consumption and a new onset of depression and generalized anxiety
disorder: Results from an international study in primary care. _Psychiatry Res._ 243, 30–34 (2016). Article PubMed Google Scholar * Schuch, F. B. & Stubbs, B. The role of exercise in
preventing and treating depression. _Curr. Sports Med. Rep._ 18, 299–304 (2019). Article PubMed Google Scholar * Sarris, J., O’Neil, A., Coulson, C. E., Schweitzer, I. & Berk, M.
Lifestyle medicine for depression. _BMC Psychiatry_ 14, 107 (2014). Article PubMed PubMed Central Google Scholar * Lopresti, A. L., Hood, S. D. & Drummond, P. D. A review of
lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. _J. Aff. Disord._ 148, 12–27 (2013). Article Google Scholar * Reid, K.
J. _et al._ Aerobic exercise improves self-reported sleep and quality of life in older adults with insomnia. _Sleep Med._ 11, 934–940 (2010). Article PubMed PubMed Central Google Scholar
* Chang, P. P., Ford, D. E., Mead, L. A., Cooper-Patrick, L. & Klag, M. J. Insomnia in young men and subsequent depression: The Johns Hopkins Precursors Study. _Am. J. Epidemiol._ 146,
105–114 (1997). Article CAS PubMed Google Scholar * Neckelmann, D., Mykletun, A. & Dahl, A. A. Chronic insomnia as a risk factor for developing anxiety and depression. _Sleep_ 30,
873–880 (2007). Article PubMed PubMed Central Google Scholar * Allan, C. E., Valkanova, V. & Ebmeier, K. P. Depression in older people is underdiagnosed. _Practitioner_ 258, 19–22
(2014). PubMed Google Scholar * Walker, J. _et al._ Major depression and survival in people with cancer. _Psychosom. Med._ 83, 410–416 (2021). Article PubMed Google Scholar * Hong, J.
S. & Tian, J. Prevalence of anxiety and depression and their risk factors in Chinese cancer patients. _Support Care Cancer._ 22, 453–459 (2014). Article PubMed Google Scholar * Irwin,
M. R. Depression and insomnia in cancer: Prevalence, risk factors, and effects on cancer outcomes. _Curr Psychiatry Rep._ 15, 404 (2013). Article PubMed Google Scholar * Savard, J. &
Morin, C. M. Insomnia in the context of cancer: A review of a neglected problem. _J. Clin. Oncol._ 19, 895–908 (2001). Article CAS PubMed Google Scholar * Kumagai, N. _et al._ Assessing
recurrence of depression using a zero-inflated negative binomial model: A secondary analysis of lifelog data. _Psychiatry Res._ 300, 113919 (2021). Article PubMed Google Scholar * Burcu,
M. _et al._ Association of antidepressant medications with incident type 2 diabetes among medicaid-insured youths. _JAMA Pediatr._ 171, 1200–1207 (2017). Article PubMed PubMed Central
Google Scholar * Bockting, C. L., Hollon, S. D., Jarrett, R. B., Kuyken, W. & Dobson, K. A lifetime approach to major depressive disorder: The contributions of psychological
interventions in preventing relapse and recurrence. _Clin. Psychol. Rev._ 41, 16–26 (2015). Article PubMed Google Scholar * Quan, H. _et al._ Coding algorithms for defining comorbidities
in ICD-9-CM and ICD-10 administrative data. _Med. Care_ 43, 1130–1139 (2005). Article PubMed Google Scholar * World Health Organization. _The ICD-10 Classification of Mental and
Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines_ (1992). Download references ACKNOWLEDGEMENTS The authors deeply acknowledge all the participants of the present study.
The authors also acknowledge Editage for providing editorial and publication support. FUNDING This research did not receive any specific grant from funding agencies in the public,
commercial, or not-for-profit sectors. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of Advanced Medicine, Nagoya University Hospital, 65 Tsuruma-cho, Showa-ku, Nagoya, Aichi,
464-8550, Japan Takahiro Imaizumi & Masahiko Ando * Department of Nephrology, Nagoya University Graduate School of Medicine, 65 Tsuruma-cho, Showa-ku, Nagoya, Aichi, 464-8550, Japan
Takahiro Imaizumi & Shoichi Maruyama * Prevent Co., Ltd., Nagoya, Japan Takuya Toda, Daisuke Sakurai & Yuta Hagiwara * Hidamari Kokoro Clinic, Ama, Japan Michitaka Maekawa *
Innovative Research Center for Preventive Medical Engineering, Nagoya University, Nagoya, Japan Yasuko Yoshida Authors * Takahiro Imaizumi View author publications You can also search for
this author inPubMed Google Scholar * Takuya Toda View author publications You can also search for this author inPubMed Google Scholar * Michitaka Maekawa View author publications You can
also search for this author inPubMed Google Scholar * Daisuke Sakurai View author publications You can also search for this author inPubMed Google Scholar * Yuta Hagiwara View author
publications You can also search for this author inPubMed Google Scholar * Yasuko Yoshida View author publications You can also search for this author inPubMed Google Scholar * Masahiko Ando
View author publications You can also search for this author inPubMed Google Scholar * Shoichi Maruyama View author publications You can also search for this author inPubMed Google Scholar
CONTRIBUTIONS T.I. analyzed the data and wrote the paper; T.T. and D.S. prepared the data; M.M., Y.H., Y.Y., M.A., and S.M. interpreted the results. CORRESPONDING AUTHORS Correspondence to
Takahiro Imaizumi or Shoichi Maruyama. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no competing interests. ADDITIONAL INFORMATION PUBLISHER'S NOTE Springer Nature
remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY INFORMATION. RIGHTS AND PERMISSIONS OPEN ACCESS
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as
long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third
party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the
article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the
copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Imaizumi, T., Toda, T.,
Maekawa, M. _et al._ Identifying high-risk population of depression: association between metabolic syndrome and depression using a health checkup and claims database. _Sci Rep_ 12, 18577
(2022). https://doi.org/10.1038/s41598-022-22048-9 Download citation * Received: 27 January 2022 * Accepted: 07 October 2022 * Published: 03 November 2022 * DOI:
https://doi.org/10.1038/s41598-022-22048-9 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative